Marcus Drake, Hashim Hashim, Andrew Gammie, Marcus Drake, Hashim Hashim, Andrew Gammie
This is a test
This is a test
Partager le livre
English
ePUB (adapté aux mobiles)
Disponible sur iOS et Android
eBook - ePub
Abrams' Urodynamics
Marcus Drake, Hashim Hashim, Andrew Gammie, Marcus Drake, Hashim Hashim, Andrew Gammie
Détails du livre
Aperçu du livre
Table des matières
Citations
À propos de ce livre
Abrams' Urodynamics
A complete guide to urodynamic investigation in modern health care
Urodynamic testing is an ever-advancing field with applications in the management of patients from across a wide range of clinical areas. Bringing together fundamental principles and cutting-edge innovations, Abrams' Urodynamics has been designed as an all-in-one guide to Functional Urology and Urogynecology, offering direct, up-to-date instruction on how to best perform and understand urodynamic tests within the overall treatment pathway. Its chapters cover everything from everyday basic practice to advanced complex cases, and are enhanced with more than 450 helpful illustrations. Including numerous revisions and new features, this fourth edition of the book boasts:
Coverage of all investigative approaches, including uroflowmetry, cystometry, video-urodynamics, and non-invasive techniques
Details on the successful running of a urodynamic unit, with information on organizational issues, equipment set-up, and common problems and pitfalls
Sections addressing children, women, men, the elderly, and neuropaths
Extensive description of International Continence Society (ICS) Standards throughout
Appendices that include ICS Standards and Fundamentals documents, ICIQ modules, and Patient Information Leaflets
With its wealth of clinical tips, illustrations, new innovations, and hands-on advice, Abrams' Urodynamics is essential reading for all those wishing to better integrate urodynamic testing into their daily practice.
Foire aux questions
Comment puis-je résilier mon abonnement ?
Il vous suffit de vous rendre dans la section compte dans paramètres et de cliquer sur « Résilier l’abonnement ». C’est aussi simple que cela ! Une fois que vous aurez résilié votre abonnement, il restera actif pour le reste de la période pour laquelle vous avez payé. Découvrez-en plus ici.
Puis-je / comment puis-je télécharger des livres ?
Pour le moment, tous nos livres en format ePub adaptés aux mobiles peuvent être téléchargés via l’application. La plupart de nos PDF sont également disponibles en téléchargement et les autres seront téléchargeables très prochainement. Découvrez-en plus ici.
Quelle est la différence entre les formules tarifaires ?
Les deux abonnements vous donnent un accès complet à la bibliothèque et à toutes les fonctionnalités de Perlego. Les seules différences sont les tarifs ainsi que la période d’abonnement : avec l’abonnement annuel, vous économiserez environ 30 % par rapport à 12 mois d’abonnement mensuel.
Qu’est-ce que Perlego ?
Nous sommes un service d’abonnement à des ouvrages universitaires en ligne, où vous pouvez accéder à toute une bibliothèque pour un prix inférieur à celui d’un seul livre par mois. Avec plus d’un million de livres sur plus de 1 000 sujets, nous avons ce qu’il vous faut ! Découvrez-en plus ici.
Prenez-vous en charge la synthèse vocale ?
Recherchez le symbole Écouter sur votre prochain livre pour voir si vous pouvez l’écouter. L’outil Écouter lit le texte à haute voix pour vous, en surlignant le passage qui est en cours de lecture. Vous pouvez le mettre sur pause, l’accélérer ou le ralentir. Découvrez-en plus ici.
Est-ce que Abrams' Urodynamics est un PDF/ePUB en ligne ?
Oui, vous pouvez accéder à Abrams' Urodynamics par Marcus Drake, Hashim Hashim, Andrew Gammie, Marcus Drake, Hashim Hashim, Andrew Gammie en format PDF et/ou ePUB ainsi qu’à d’autres livres populaires dans Médecine et Hématologie. Nous disposons de plus d’un million d’ouvrages à découvrir dans notre catalogue.
Marcus Drake1, Andrew Gammie2, Laura Thomas3, Arturo García‐Mora4, and Hashim Hashim2
1 Translational Health Sciences, Bristol Medical School, Southmead Hospital, Bristol, UK
2 Bristol Urological Institute, Southmead Hospital, Bristol, UK
3 Urodynamics & Gastrointestinal Physiology, Southmead Hospital, Bristol, UK
4 Instituto Nacional de Ciencias Médicas y Nutrición “Salvador Zubirán”, Hospital Médica Sur, Mexico City, México
Introduction to Urodynamics
Urodynamics has two basic aims:
To reproduce the patient's symptomatic complaints while making key observations
To provide a pathophysiological explanation by correlating the patient's symptoms with the urodynamic findings
These two basic aims are crucial to the purpose of urodynamics – essentially, it is a diagnostic test that will aid in the management of patients. The need to make urodynamic observations reflects the fact that the patient's symptoms are important, but they might be somewhat misleading. Most patients with lower urinary tract dysfunction (LUTD) present to their doctor with symptoms. However, lower urinary tract symptoms (LUTS – Table 1.1) should not simply be taken at face value, since a range of differing mechanisms may result in rather similar symptomatic presentations. The statement ‘the bladder is an unreliable witness’ [2] reflects how symptoms are the starting point but do not actually identify the ultimate explanation. Since treatment should correct the underlying cause, it is necessary to identify mechanisms, avoiding assumption or prejudice coming from taking symptoms at face value. An excellent example of this is voiding LUTS in men, where the cause on urodynamic testing may prove to be bladder outlet obstruction (BOO) and/or detrusor underactivity (DUA); BOO should respond fully to surgery to relieve obstruction such as transurethral resection of prostate (TURP), while such surgery is potentially not helpful in the second [3]. Voiding LUTS in males are of unreliable diagnostic value, and only slow stream and hesitancy show any correlation with the urodynamic findings of BOO [4–6]. Even with flow rate assessment, one cannot be sure whether BOO is present (Figure 1.1). The difficulty of assessing LUTD by symptoms alone is the uncertainty about establishing truly what is going on in the individual describing them.
Table 1.1 Classification of lower urinary tract symptoms (LUTS) [1].
Source: Modified from Abrams et al. [1].
Storage
Voiding
Post‐micturition
Urgency
Slow stream
Post‐micturition dribbling
Urinary incontinence
Splitting/spraying
Feeling of incomplete emptying
Increased daytime frequency
Intermittency
Nocturia
Hesitancy
Pain
Straining
Terminal dribbling
Note: Do NOT forget to enquire about Pelvic Organ Prolapse in Women and Erectile Dysfunction in Men.
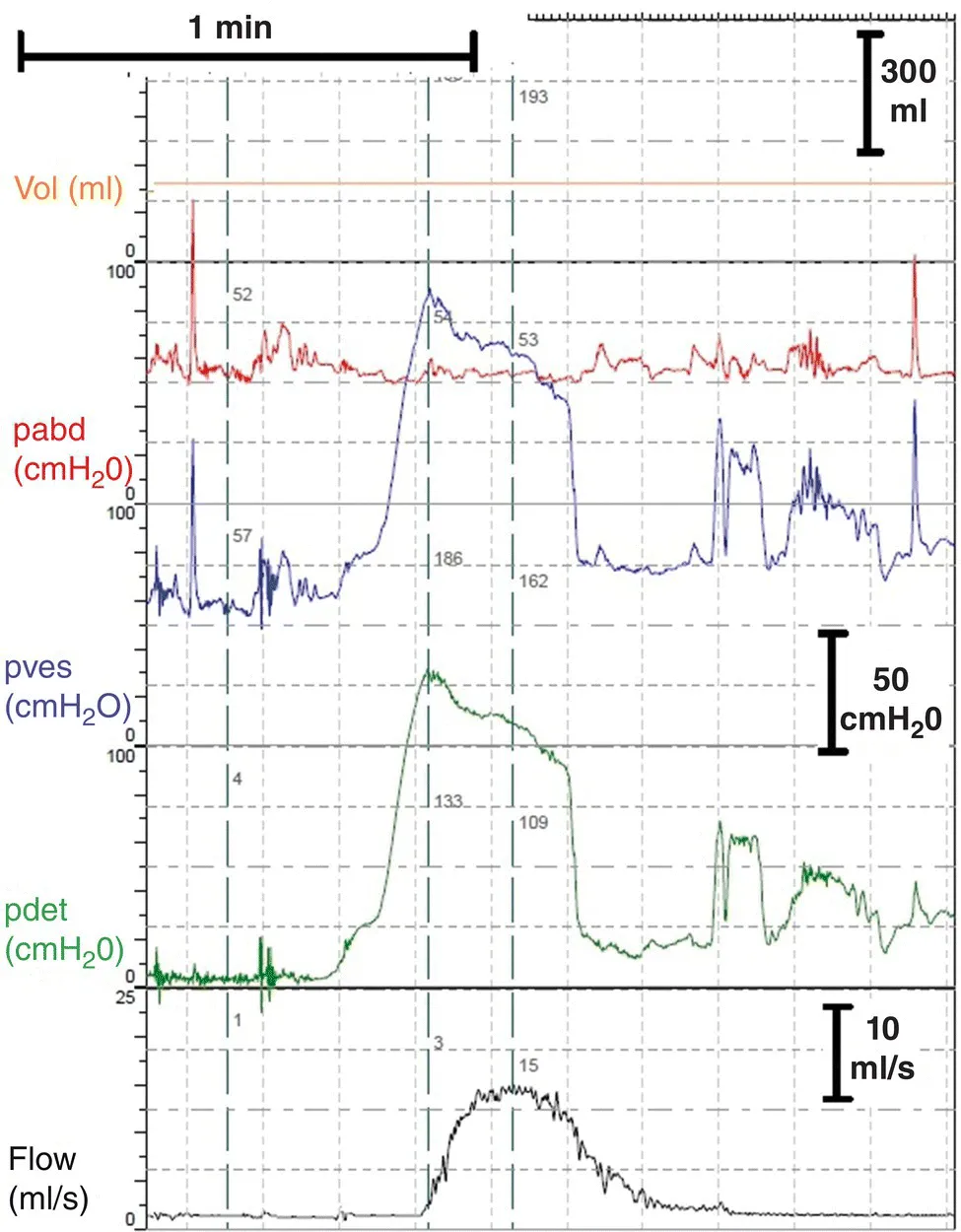
Figure 1.1 Flow rate testing in men gives an uncertain understanding. This man had previously done a free flow rate test which showed a reasonable maximum flow rate of 16 ml/s; taken alone, this might suggest he does not have bladder outlet obstruction (BOO). However, when he attended for urodynamics (see the pressure‐flow study illustrated above), his flow rate was 15 ml/s as shown, but the pressure needed to achieve this was high, indicating BOO is present (see Chapter 14 for more details on assessing BOO in men).
For women diagnosed by their symptoms as having stress urinary incontinence (SUI), only 50–68% have urodynamic stress incontinence (USI) [7, 8]. These studies also looked at patients with apparent overactive bladder (OAB) symptoms presumed to be the result of detrusor overactivity (DO), and here, the correspondence was 33– 51%. A key factor is the link to coughing, often used as a question to elicit a history of SUI; if a woman says ‘I leak when I cough’, it sounds like SUI. However, a cough can be a trigger to set off an overactive detrusor contraction, leading to detrusor overactivity incontinence (DOI) (Figure 1.2). Thus, the history may suggest that SUI treatment is needed, but for some of these women, the urodynamic observation identifies that DO treatment is the appropriate choice.
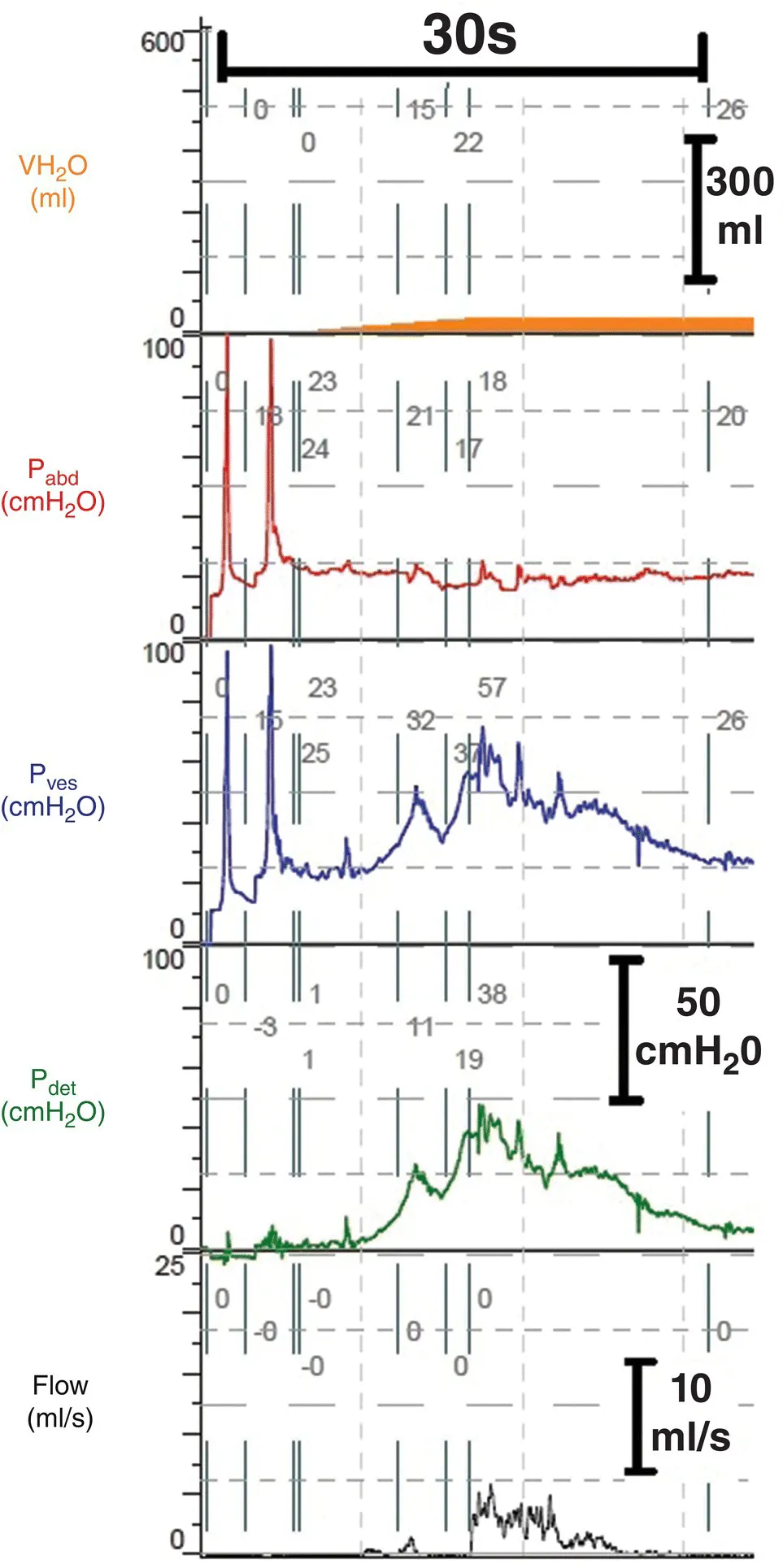
Figure 1.2 A woman who reported leakage with coughing in her history, suggestive of stress urinary incontinence (SUI). Her urodynamic test showed cough‐provoked detrusor overactivity (DO) incontinence, and she described this as representative of her presenting complaint. Hence, this is not urodynamic stress incontinence, but effort‐provoked detrusor overactivity incontinence; the symptomatic presentation was misleading and could have led to inappropriate surgery for SUI (see Chapter 13 for more details on assessing incontinence in women).
Accordingly, in both men and women, there is potential mismatch between reported LUTS and the LUTD identified by detailed investigation. This issue is particularly prominent in people with neurological conditions and children. In neurological disease, it is common for sensation to be absent or abnormal, making LUTS even more difficult to interpret. Children may find it difficult to des...