Ultrasound of the Diaphragm and the Respiratory Muscles
Massimo Zambon, Massimo Zambon
This is a test
This is a test
152 pages
English
ePUB (adapté aux mobiles)
Disponible sur iOS et Android
eBook - ePub
Ultrasound of the Diaphragm and the Respiratory Muscles
Massimo Zambon, Massimo Zambon
Détails du livre
Aperçu du livre
Table des matières
Citations
À propos de ce livre
Ultrasound is the most reliable, easily available, fast, non-invasive technique to study diaphragm function, and is an irreplaceable tool to diagnose, monitor, and follow -up critical respiratory patients. This essential guide analyses every aspect of ultrasound of the diaphragm and respiratory muscles, a reliable assessment whose function is vital to delivering the most suitable treatment. Ultrasound of the Diaphragm and the Respiratory Muscles also provides insight to diagnosing diaphragmatic dysfunction or paralysis following surgery or neuromuscular diseases, to follow the muscular activity and the time-course of atrophy during mechanical ventilation, and to monitor the weaning phase. It is ideal for professionals and trainees practicing ultrasound in a clinical setting.
Key Features
Sets the standard for training and competency of this emerging, yet scientifically approved non-invasive technique of ultrasound with all the essential information on how to perform ultrasound and interpret the images obtained.
Features clear and didactic images demonstrating echo findings in various situations along with videos of diaphragmatic ultrasound offering a unique "window" on mechanically ventilated patients, allowing to take important clinical decisions on ventilatory modes and assistance by pulmonologists, critical care specialists, thoracic surgeons, emergency medicine specialists, as well as trainees.
Includes a chapter on paediatric ultrasound along with ultrasound of other respiratory muscles (i.e., intercostal and abdominal) which is emerging as a useful complementary tool.
Foire aux questions
Comment puis-je résilier mon abonnement ?
Il vous suffit de vous rendre dans la section compte dans paramètres et de cliquer sur « Résilier l’abonnement ». C’est aussi simple que cela ! Une fois que vous aurez résilié votre abonnement, il restera actif pour le reste de la période pour laquelle vous avez payé. Découvrez-en plus ici.
Puis-je / comment puis-je télécharger des livres ?
Pour le moment, tous nos livres en format ePub adaptés aux mobiles peuvent être téléchargés via l’application. La plupart de nos PDF sont également disponibles en téléchargement et les autres seront téléchargeables très prochainement. Découvrez-en plus ici.
Quelle est la différence entre les formules tarifaires ?
Les deux abonnements vous donnent un accès complet à la bibliothèque et à toutes les fonctionnalités de Perlego. Les seules différences sont les tarifs ainsi que la période d’abonnement : avec l’abonnement annuel, vous économiserez environ 30 % par rapport à 12 mois d’abonnement mensuel.
Qu’est-ce que Perlego ?
Nous sommes un service d’abonnement à des ouvrages universitaires en ligne, où vous pouvez accéder à toute une bibliothèque pour un prix inférieur à celui d’un seul livre par mois. Avec plus d’un million de livres sur plus de 1 000 sujets, nous avons ce qu’il vous faut ! Découvrez-en plus ici.
Prenez-vous en charge la synthèse vocale ?
Recherchez le symbole Écouter sur votre prochain livre pour voir si vous pouvez l’écouter. L’outil Écouter lit le texte à haute voix pour vous, en surlignant le passage qui est en cours de lecture. Vous pouvez le mettre sur pause, l’accélérer ou le ralentir. Découvrez-en plus ici.
Est-ce que Ultrasound of the Diaphragm and the Respiratory Muscles est un PDF/ePUB en ligne ?
Oui, vous pouvez accéder à Ultrasound of the Diaphragm and the Respiratory Muscles par Massimo Zambon, Massimo Zambon en format PDF et/ou ePUB ainsi qu’à d’autres livres populaires dans Medicina et Medicina polmonare e toracica. Nous disposons de plus d’un million d’ouvrages à découvrir dans notre catalogue.
1 Anatomy, Physiology, and Dysfunction of the Diaphragm
Marco Gemma
DOI: 10.1201/9781003128694-2
Anatomy
Physiology
Dysfunction
References
In evolution, the diaphragm muscle is unique to mammals, and its physiological importance cannot be argued (1).
Anatomy
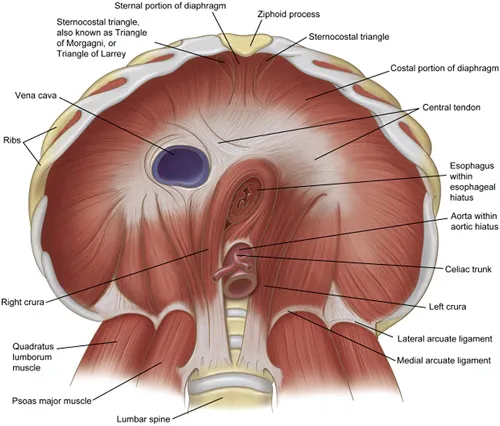
The diaphragm is a dome-shaped 2–4 mm thick muscular sheet that separates the thoracic and the abdominal cavities (2–5) (Figure 1.1).
Figure 1.1 The anatomy of the normal diaphragm. Reproduced with permission from ref. 4 (Downey R, Anatomy of the normal diaphragm, Thorac Surg Clin 21(2) (2011) 273–79). Anatomy of the diaphragm
Actually, the diaphragm is formed by two muscle bellies (domes or cupolae) connected at the level of the xiphosternal joint by the central tendon. This flat non-contractile collagen aponeurosis provides support to the heart, whereas the right and the left cupolae support the corresponding lungs. The apex of the diaphragm ranges widely in height during the breathing cycle (even between the fourth rib and the costal margin) depending on breathing depth, body posture, and abdominal pressure. The right cupola, lying above the liver, reaches a 2–3 cm higher level than the left one.
The diaphragm muscle fibres arise from the inner aspect of the thoracic cage (4 –9).
Posteriorly, the diaphragm muscle fibres are organized in two paired crura, which originate from the anterior aspects of L1–L3 and are joined by the median arcuate ligament. Hypertrophy or lower displacement of this fibrous structure may cause the median arcuate ligament syndrome (MALS, also known as celiac artery compression syndrome, celiac axis syndrome, celiac trunk compression syndrome, or Dunbar syndrome).
More anteriorly, the diaphragm muscle fibres rise from the paired medial arcuate ligaments, which join the vertebral tendinous origin of the respective diaphragmatic crus to the transverse processes of L1 or L2, after covering the anterior surface of the major psoas muscle. Even more anteriorly, the muscle fibres take origin from the paired lateral arcuate ligaments, which spread from the transverse processes of T12–L3 (variably) to the mid portion of the twelfth ribs covering the quadratus lumborum muscle. All these arcuate ligaments are thickened fascial bands that are sometimes mistaken for pathological structures on clinical imaging.
Antero-laterally and anteriorly, the cupolae are formed by muscle fibres originating from the inner surface of the lower six ribs and of the xiphoid process, respectively.
From their origin inside the rib cage the diaphragm muscle fibres direct cephalad and are substantially vertical. They gradually horizontalize, producing the aforementioned dome shape of the muscle. In this setting, the distal part of the diaphragmatic dome abuts the lower rib cage from the costal insertion to a point referred to as costophrenic angle. This portion is known as the zone of apposition (ZOA) (10, 11).
During quiet breathing the ZOA is one-quarter to one-third of the total inner rib cage area.
A number of ligaments connect the diaphragm to neighbouring viscera (5).
The inferior pulmonary ligament, the phrenopericardial ligament, the falciform and the paired triangular ligaments of the liver, the phrenicoesophageal ligament, and the phrenicocolic ligament (to the angle of the ascending colon) are pleural, pericardial, or peritoneal thickening.
The ligament of Treitz is made up of muscle fibres from the left crus reaching the duodenojejunal angle.
Three hiatuses allow passage between the thoracic and the abdominal cavities (5, 12).
The caval hiatus, at the T8 level, in the middle of the central tendon, is traversed by the inferior vena cava and some branches of the right phrenic nerve. It enlarges during inspiration, favouring blood flow to the heart.
The oesophageal hiatus, at the T10 level, through the right crus, allows passage to the oesophagus, the vagus nerve, and some sympathetic nerve branches. It works as a muscular sphincter, constricting during inspiration and preventing gastroesophageal reflux.
The aortic hiatus, at the T12 level, beyond the crura, transmits the aorta, the thoracic duct and the azygos and hemiazygos veins. It is unaffected by diaphragmatic contraction.
Several smaller and inconstant apertures in the diaphragm allow the passage of blood and lymph vessels.
The superior surface of the diaphragm receives its blood supply from branches of the internal thoracic mammary artery (the musculophrenic, pericardiacophrenic, and superior epigastric arteries) and of the lower thoracic aorta (phrenic branches), besides. the lower five intercostal and subcostal arteries.
The inferior surface is supplied by branches of the abdominal aorta or of the coeliac trunk (inferior phrenic arteries) (5).
The venous drainage strictly mirrors the arterial supply. Eventually the superior surface veins drain into the internal thoracic vein and the inferior surface veins drain into the inferior vena cava (right hemidiaphragm) and the renal or suprarenal left vein (left hemidiaphragm).
Both diaphragmatic surfaces are covered by lymph plexuses anastomosing with each other and with pleural and peritoneal lymphatics. Retrosternal, perioesophageal/caval, and periaortic lymph nodes receive the lymphatic drainage, respectively, from the anterior, middle, and posterior third of the diaphragm (5).
Motor innervation comes to the diaphragm exclusively through the paired phrenic nerves. Except for a small contribution from the sixth or seventh intercostal nerves, the phrenic nerves provide also the sensitive innervation (5, 13–15).
The phrenic nerves rise from the ventral horn (lamina IX) of C3–C5. They reach the diaphragm laterally to the inferior vena cava on the right and laterally to the heart on the left and then divide in several branches inside the muscle thickness. The innervation of the two hemidiaphragms is ipsilateral and even the crural fibres are supplied by the ipsilateral phrenic nerve, regardless of their side of origin but according to their course to the right or left of the oesophageal opening. The innervation is somatotopic, since more rostral medullary segments innervate more ventral diaphragmatic portions (16, 17).
The phrenic motor neurons are monosynaptically innervated by pre-motor neurons lying in the ventro-lateral and dorso-me...
Table des matières
Normes de citation pour Ultrasound of the Diaphragm and the Respiratory Muscles
APA 6 Citation
Zambon, M. (2022). Ultrasound of the Diaphragm and the Respiratory Muscles (1st ed.). CRC Press. Retrieved from https://www.perlego.com/book/3295197/ultrasound-of-the-diaphragm-and-the-respiratory-muscles-pdf (Original work published 2022)
Chicago Citation
Zambon, Massimo. (2022) 2022. Ultrasound of the Diaphragm and the Respiratory Muscles. 1st ed. CRC Press. https://www.perlego.com/book/3295197/ultrasound-of-the-diaphragm-and-the-respiratory-muscles-pdf.
Harvard Citation
Zambon, M. (2022) Ultrasound of the Diaphragm and the Respiratory Muscles. 1st edn. CRC Press. Available at: https://www.perlego.com/book/3295197/ultrasound-of-the-diaphragm-and-the-respiratory-muscles-pdf (Accessed: 15 October 2022).
MLA 7 Citation
Zambon, Massimo. Ultrasound of the Diaphragm and the Respiratory Muscles. 1st ed. CRC Press, 2022. Web. 15 Oct. 2022.