![]()
Chapter 1
Ophthalmic Formulation
CLIVE G. WILSONa
a Strathclyde Institute of Pharmacy & Biomedical Sciences, Glasgow, U.K Email:
[email protected] 1.1 Introduction
Poor sight constitutes a major and expensive burden to society, with risk of accidental self harm, the need for specialised provision and often the extensive involvement of family members in care. Sight loss arises from trauma, disease, infection and old age, with thinning of the retinal nerve fibre layers at a rate of 3 µm per decade or 0.27% per year over an age range of 18 to 80 years.1 Some diseases of old age such as cataracts are now routinely treated but as we live longer, the principal eye diseases in the Western world impact the elderly population. These ocular conditions include age-related macular degeneration, diabetic retinopathy and glaucoma.
In ophthalmic medicine, the scope for intervention is uniquely difficult as the structures defend the inner target – the retina, by the blood–retina barriers preventing penetration of drugs circulating in the systemic circulation and the outer tissues preserve ocular acuity by attempting to dilute and wipe away any medicine applied topically by blinking. The eyes are vulnerable anatomically, and recently it has been hypothesised that COVID might be spread by droplet to eye surface contact. This suggests that the wearing of glasses might be a simple protective measure against aerosol-borne infection.
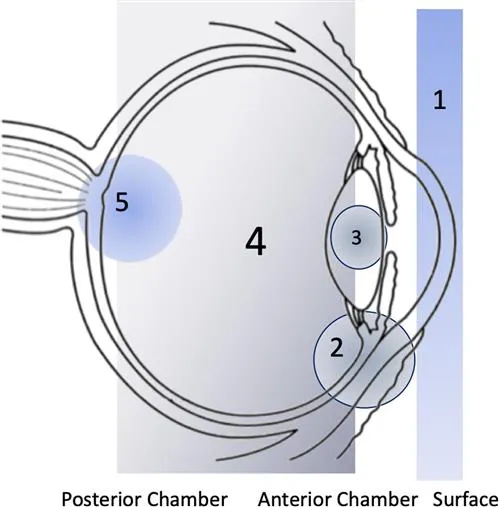
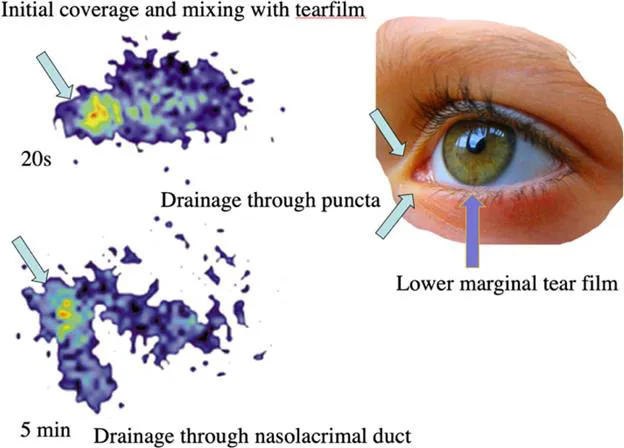
The internal drug delivery targets are shown in Figure 1.1. Following administration of a topical formulation, the drop mixes with the tear film and is drained through the nasolacrimal apparatus (Figure 1.2). The drainage from the eye moves drug through the facial viscera with venous return ultimately to the heart. Modern delivery systems for ocular drug treatment must therefore serve the following tasks: sustained efficacy, residence without blurring, increased transport without hyperaemia and minimisation of side effects especially cardiovascular insult. For the eye, packaging systems are also important as those for daily use must remain clean, stable and appropriate for use.
Figure 1.1 Showing targets for treatment.
Figure 1.2 Application to the tear film leads to rapid drainage through the nasolacrimal duct as illustrated by lacrimal scintigraphy following instillation of [99mTc]-labelled aqueous formulation onto the eye surface.
The usual technique of dosing is to pull down the lid to make a pocket to accommodate the drop and therefore most formulations encounter the mucous layer of the conjunctivae rather than the cornea. Patients should be trained to achieve safe and effective dosing but often will apply multiple drops. The excess is lost through the nasolacrimal duct or spillage on the cheek. On relaxing the pinch, the lid closes, expelling most of the dose. The reflex tearing mechanism, activated by the change in surface temperature and a few seconds later by the drop composition, further dilutes the formulation.
The globe protrudes from the skull and the eye is very vulnerable. Additionally, the wet surface is prone to desiccation and accumulates particulate matter which must be cleared to maintain visual acuity. This is because the lens and wet cornea form a compound lens structure, with the cornea providing about 43 dioptres and the lens 16 dioptres. The dioptre is the unit of refractive power equal to the reciprocal of the focal length of a given lens. The addition of a drop of liquid to the cornea therefore causes a large change in refraction and triggers blinking and a reflex upward movement of the eye. The pull back on the blink generates negative pressure in the lacrimal sac, assisting the flow of tears from the gland. The blink compresses the tear film and the thickness of the film increases, and the eye no longer focuses an image.
1.2 The Tear Film
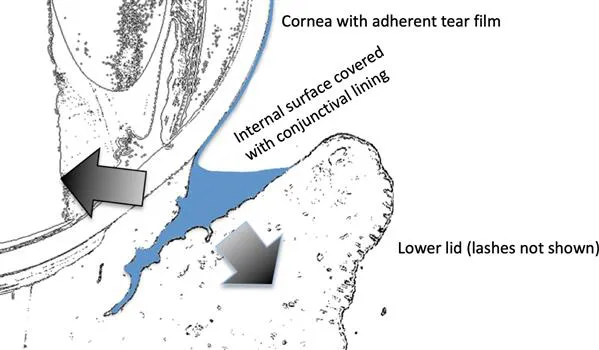
Tears are secreted through the lacrimal gland and supplemented by lipids provided by the Meibomian glands. The film is adherent and very thin over the cornea (thickness 2–5.5 µm), as illustrated in Figure 1.3. Note that the lower marginal strip acts as a reservoir for the applied drop. Mucin is secreted by the lacrimal gland and to a lesser extent the goblet cells of the conjunctivae. The mucin gel is composed of heavily O-glycosylated protein domains making up 50–80% of the weight of the mucin. This carbohydrate/protein structure increases adherence and without adequate mucin the tear film is unstable. The tear film is then unable to wet the surface, promoting the formation of dry spots which can become a difficult problem to treat. The mucins, being thixotropic, allow stability at rest and shear thinning during blinking. Overall, this provides protective and lubricative functions but tears are variable in composition. Basal flow provides the resting coat but reflex tears are produced by contact stimulation or blowing the nose. Emotional tears are also produce by central arc stimulation and have higher protein content than reflex tears2 as do closed-eye tears collected after sleeping. This is due to the serum content produced by leakage of the conjunctival blood vessels. The rate of tear secretion, estimated at between 0.5 and 2.2 µL min−1, is affected by environmental conditions, age, disease and psychological state.3 Osmolarity of the tear film is estimated as 290–310 mOsm kg−1 in healthy adults, rising to 320–325 mOsm kg−1 in dry eye disease.
Figure 1.3 The lower marginal strip acts as a reservoir for conjunctival absorption.
The pH of freshly secreted normal tears is measured at 7.2–7.4 but old studies of contact lens wearers who wore rigid lenses suggest that the tear film can be more acidic (pH 6.6) due to the build up of carbon dioxide under the lens.4 Similarly, pH is lowest on awakening as a result of acid by-products associated with relatively anaerobic conditions in prolonged lid closure and pH increases because of loss of carbon dioxide as the eyes open. The same authors found disease in non-contact wearers can make the tear film more alkaline. The chemical composition of tears was reviewed by Tiffany, who with Prof. Bron, made great advances in understanding the nature of the tear film.5 Tiffany measured tear viscosity and described the film as weakly elastic due to the lipid layer. He measured values of 4.4–8.3 mPa seconds for normal tears and 28–31 mPa seconds in patients with dry eye. An excellent description of the solids which constitute 1.8% of the tear film was given in a recent e-book.6
Meibomian glands are situated at the base of the lashes and secrete a lipid mix of phospholipids, neutral oils, sterol esters and other waxy lipids with a melting point range of 19–32 °C.7,8 Branched and unsaturated lipids are responsible for a lowering of the melting point.9 The tear film lipid layer can be observed by interferometry and is approximately 40 nm thick and extends upwards over the film to the gland like a curtain, travelling upwards during the upswing of a blink. The instillation of a solution containing drugs or adjuvants that lower the surface tension may disrupt the outermost lipid of the tear film into oily droplets, which become solubilized. The protective effect of the oily film against evaporation of the tear film aqueous layer will then disappear. Approximately 3 µL of a solution can be incorporated in the precorneal film without causing it to destabilise. Alteration in the resident tear film can be noted by a change in the tear break-up time when the tears are stained with fluorescein. Alteration in the composition of tears, usually a change in mucin or lipid composition, results in decreased wettability and faster tear evaporation, leading to painful dry spots on the cornea or “dry eye disease”.10 Wetting agents are often added to dry eye treatment drops to improve contact on a surface that with drying becomes more hydrophobic.
The eye is not a portal for systemic delivery although topical delivery to the eye can result in profound systemic effects; for example, the administration of a beta blocker to exercising students decreased heart rate11 and the effects in other adult groups was markedly affected by formulation.12 Generally the purpose of ocular delivery is to treat that organ, albeit that dosing can be ineffective. Missing the target and missing the opportunity to treat are common problems in ophthalmic medical practice.13 The issue of comfort and lack of fuss in the dosing becomes important in silently advancing diseases such as glaucoma because, as far as the patient is concerned, there is no signal of immediate benefit.
1.3 Delivery Volume and the Dosing Device
Diseases affecting the front of the eye can often be treated topically which, as ophthalmic solutions are easy to pre...