
eBook - ePub
Practical Obstetrics
Joachim W. Dudenhausen, Susan E. Travis
This is a test
Partager le livre
- 511 pages
- English
- ePUB (adapté aux mobiles)
- Disponible sur iOS et Android
eBook - ePub
Practical Obstetrics
Joachim W. Dudenhausen, Susan E. Travis
Détails du livre
Aperçu du livre
Table des matières
Citations
À propos de ce livre
The 21st edition of this standard reference book – now published in English for the first time – provides indispensable, hands-on information for the delivery room, as well as before and after childbirth. The book combines proven facts and techniques with new insights through a consistent focus on practical and applied knowledge. All of those involved in the care of pregnant, laboring, and postnatal women and newborn can benefit from the established didactic concept of this book.
Foire aux questions
Comment puis-je résilier mon abonnement ?
Il vous suffit de vous rendre dans la section compte dans paramètres et de cliquer sur « Résilier l’abonnement ». C’est aussi simple que cela ! Une fois que vous aurez résilié votre abonnement, il restera actif pour le reste de la période pour laquelle vous avez payé. Découvrez-en plus ici.
Puis-je / comment puis-je télécharger des livres ?
Pour le moment, tous nos livres en format ePub adaptés aux mobiles peuvent être téléchargés via l’application. La plupart de nos PDF sont également disponibles en téléchargement et les autres seront téléchargeables très prochainement. Découvrez-en plus ici.
Quelle est la différence entre les formules tarifaires ?
Les deux abonnements vous donnent un accès complet à la bibliothèque et à toutes les fonctionnalités de Perlego. Les seules différences sont les tarifs ainsi que la période d’abonnement : avec l’abonnement annuel, vous économiserez environ 30 % par rapport à 12 mois d’abonnement mensuel.
Qu’est-ce que Perlego ?
Nous sommes un service d’abonnement à des ouvrages universitaires en ligne, où vous pouvez accéder à toute une bibliothèque pour un prix inférieur à celui d’un seul livre par mois. Avec plus d’un million de livres sur plus de 1 000 sujets, nous avons ce qu’il vous faut ! Découvrez-en plus ici.
Prenez-vous en charge la synthèse vocale ?
Recherchez le symbole Écouter sur votre prochain livre pour voir si vous pouvez l’écouter. L’outil Écouter lit le texte à haute voix pour vous, en surlignant le passage qui est en cours de lecture. Vous pouvez le mettre sur pause, l’accélérer ou le ralentir. Découvrez-en plus ici.
Est-ce que Practical Obstetrics est un PDF/ePUB en ligne ?
Oui, vous pouvez accéder à Practical Obstetrics par Joachim W. Dudenhausen, Susan E. Travis en format PDF et/ou ePUB ainsi qu’à d’autres livres populaires dans Medicine et Perinatology & Neonatology. Nous disposons de plus d’un million d’ouvrages à découvrir dans notre catalogue.
Informations
1 Physiology
Definitions
Ovulation. Release of the ovum from the ovary on day 14 of the menstrual cycle of a woman of child-bearing age. The oocyte is flushed out of the Graafian follicle with the follicular fluid and consists of egg plasma with core, nucleolus, and zona pellucida. It is surrounded by follicular epithelial cells (corona radiata) and enters the fallopian tube through the fimbrial end. The passage of the ovum through the fallopian tube into the uterus takes five days.
Copulation. Sexual intercourse, cohabitation, coitus; copulation is coitus performed for the purpose of reproduction. The ejaculate (approx. 4 ml), containing 200 million sperm, is deposited in the posterior fornix. From there the sperm swim through the cervical mucus and the uterus to the entrance of the fallopian tube.
Conception. Coitus resulting in fertilization; fusion of ovum and spermatozoa in the ampulla of the fallopian tube.
Extrauterine fertilization (such as in the abdomen, the ovary or a section of the fallopian tube) may occur in cases of abnormal transport of the ovum to the uterine cavity.
Fertile period. The oocytes remain fertile for six to eight hours. Sperm can live for up to two days. The fertile period of the menstrual cycle is four days.
There are two fertile phases: impregnation and conjugation
- – Impregnation (Fig. 1.1). The sperm penetrates the ripe ovum, thus creating a fertilized cell (zygote). The egg cytoplasm shrinks as a result of the sperm penetration, creating the perivitelline space between the zona pellucida and the ooplasm.
- – Conjugation. Fusion of the nuclei of sperm and ovum; fusion of the chromosomes of the pronuclei on day one-two. They line up on the equatorial plane without fusing. Fertilization is now complete.
Cleavage. The development of grooves on the surface of the fertilized ovum, visible sign of cell division on day two to three after conception. Continued cell division results in the creation of many daughter cells.
Morula (Latin for mulberry). A ball of daughter cells or blastomeres, reaching the 16-cell stage on day three to five.
Blastocyst. Conceptus, product of conception. On day five the intercellular spaces enlarge and cavitation occurs, resulting in the creation of the blastocyst cavity. The morula becomes the blastocyst, consisting of the trophoblast, the outer cell layer, which develops into the chorionic epithelium (the fetal epithelium part of the placenta), and the embryoblast, or inner cell mass. The embryoblast develops into the embryo, amnion, yolk sac, allantois, and the chorionic mesoderm (fetal connective tissue part of the placenta).
Nidation, implantation. The blastocyst embeds itself in the endometrial wall of the uterus (decidua), which has been prepared for the pregnancy, on day six or seven after lysis of the zona pellucida has occurred.
Microvilli emerge from the endometrial cells and transform into smooth epithelial cells of the uterus (pinopods). These cells increase in size through the absorption of fluids from the uterine cavity and the influence of progesterone. Estrogens stimulate the release of the adhesive molecule Mucin 1, which facilitates the implantation of the blastocyst. The invasion of the implanted blastocyst is directed by interleukins, cytokines, and interferons. This leads to a production cascade of vascular endothelial growth factor (VEGF), nitric oxide, and prostacyclins.
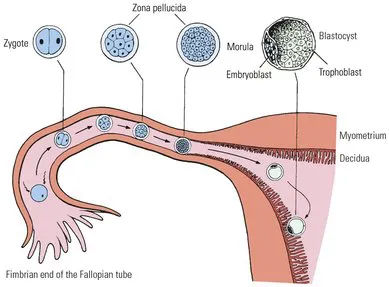
Fig. 1.1 : Development of the fertilized ovum before implantation.
Invading trophoblast. The cells of the implanted trophoblast surrounding the embryoblast erode the uterine epithelium with the help of enzymes, allowing it to embed in the endometrium, where rapid cell proliferation occurs. Some of the substances released in the process nourish the conceptus (histiotrophic phase). Numerous maternal blood vessels are eroded, and the first contact with maternal blood occurs. In this way the primitive maternal intervillous capillary system is constructed within the trophoblast. The histiotrophic phase is completed on days nine to twelve, and the hemotrophic phase begins.
Absorption trophoblast. Differentiation of the trophoblast; the intercellular boundaries fuse in the peripheral trophoblastic cells, forming the syncytium (syncytiotrophoblast), while the inner trophoblastic cells (those closest to the embryo) retain their cellular form (cytotrophoblast, Langhans cell layer). Fingerlike projections grow from the cytotrophoblast into the syncytium, forming the primary chorionic villi.
Amniotic cavity. A gap forms in the originally solid embryoblast. The base of this gap is formed by the epiblast; the top by the amniotic layer of the embryoblast (hypoblast).
Formation of the germ layers (Fig. 1.2). The embryonic shield differentiates into the three germ layers: ectoderm, endoderm, and mesoderm.
- – The ectodermal layer gives rise to the nervous system, skin, hair, nails, eyes, and ears.
- – The mesodermal layer gives rise to bones, muscles, connective tissue, vessels, and the urogenital system.
- – The endodermal layer gives rise to the gastrointestinal tract, liver, bile system, pancreas, thyroid, and lungs. The endoderm grows over the edge of the embryoblast into the inner cytotrophoblast until it surrounds a cavity: the yolk sac.
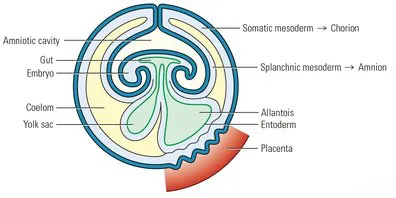
Fig. 1.2: Embryo three weeks after conception.
Extraembryonic mesoderm. Reticulum-like tissue which develops from the cells surrounding the embryoblast. In the 15-day-old embryo it covers the two close vesicles: the amniotic cavity and the yolk sac. It thickens to make up the chorion (somatic mesoderm) on the inner side of the trophoblast and on the outer side of the embryo the amnion, (sphlanchnic mesoderm).
Body stalk. Mesenchymal strand at the caudal end of the embryo, connecting chorion and amnion, later developing into the umbilical cord. The first blood vessels develop in the body stalk and in the mesoderm (blood islands and cells) on week three of embryonic development. The allantois follows, as part of the developing hindgut. During this rudimentary development, the blood vessels of the allantois penetrate the body stalk and later become the umbilical vessels.
Trophoblast invasion. Trophoblastic cells migrate into the decidua and the inner third of the myometrium to anchor the placenta and increase uteroplacental perfusion by remodeling the spiral arterioles. These trophoblastic cells are known as extravillous trophoblasts (in contrast to the villous trophoblast = placental villi). Extravillous trophoblasts take one of two paths:
- – Interstitial invasion. Trophoblasts migrate from the villi into the decidua and myometrium, secreting an extra-cellular matrix which anchors the placenta in the decidua. They cause endothelial swelling in the spiral arterioles, edema, and a reduction of elasticity.
- – Endovascular invasion. From week 10, trophoblasts are found in place of the intima and in the media of the spiral arteriole...