![]()
Chapter 1
McLaren DS, Kraemer K (eds): Manual on Vitamin A Deficiency Disorders (VADD).
World Rev Nutr Diet. Basel, Karger, 2012, vol 103, pp 1-6
______________________
Foreground
The story of how the complex of disorders of human health now known as Vitamin A Deficiency Disorders (VADD) came to be recognized over the course of time is a truly remarkable one. Detailed accounts have been published in recent years (McLaren 1999 and 2004a). Table 1.1 provides the dates of key events in the story.
It is intended that detailed and up-to-date information on every relevant aspect of VADD will be systematically covered in the chapters that follow, with attention being focused in particular on providing an outline of their setting, nature, and significance. This outline is meant to introduce the subject in such a way that a degree of confidence, involvement and concern is instilled in the reader from the outset.
Setting of VADD
Vitamin A deficiency is just one among many vitamin deficiencies that occur in humans. The form that damages the eye and vision, known as xerophthalmia, has been documented since ancient times. Other vitamin deficiencies, similarly long since recorded, include beriberi (thiamine deficiency), pellagra (niacin deficiency), scurvy (vitamin C deficiency), rickets and osteomalacia (vitamin D deficiency).
Vitamins and certain minerals make up the micronutrients - substances required for health in very small amounts, i.e. just a few milligrams or micrograms per day. There are also several lipids, known as essential fatty acids, which are needed in the diet in small amounts.
Finally, there are macronutrients, the fats, proteins, and carbohydrates needed in relatively large amounts to help provide the body with energy and fulfil its structural requirements. Some of the building blocks of proteins, amino acids, are ‘essential’ nutrients.
Varying combinations of deficiencies in all these substances lead to what is probably the most widespread nutritional deficiency disease of all: protein-energy malnutrition (PEM). In its most severe clinical forms this syndrome includes kwashiorkor and marasmus, but the majority of cases are characterized by failure to thrive and underweight.
The latest press release on global young child annual mortality data is that of UNICEF (10 September 2009). According to these data the absolute number of child deaths in 2008 declined to an estimated 8.8 million, from 12.5 million in 1990. The data show that global under-five mortality has decreased steadily over the past two decades. The average rate of decline from 2000 to 2008 is 2.3%, compared to a 1.4% average decline from 1990 to 2000.
Table 1.1. Historical background
| 1816 | Xerophthalmia in experimental animals |
| 1904 | First large human epidemic in Japan |
| 1913 | ‘Fat soluble A’discovered in the USA |
| 1930 | Formulae of β-carotene and vitamin A discovered (Karrer, Switzerland) |
| 1947 | Industrial vitamin A synthesis (Isler at Roche, Switzerland) |
| 1964 | First global survey of VADD |
| 1980s | Importance of vitamin A in child survival shown |
| 1990s | Maternal mortality reduced with retinol or β-carotene supplements Discovery of retinoid receptor gene family |
Table 1.2. Major nutritional deficiency diseases
| 1 | Protein-Energy Malnutrition (PEM) |
| 2 | Vitamin A Deficiency Disorders (VADD) |
| 3 | Nutritional Anemias (especially Iron) |
| 4 | Iodine Deficiency Disorders (IDD) |
| 5 | Zinc Deficiency |
Table 1.2 lists the five main nutritional deficiency diseases. When the WHO first named four major deficiency diseases as being of global public health magnitude (Anon 1972), zinc deficiency in humans had been barely recognized (see Chapter 10). It is rather depressing to have to note that after more than 30 years the original four deficiency diseases still remain major problems and have been joined by a fifth.
More than a third of all children under the age of five in developing countries are affected by PEM: by international criteria they are either wasted, stunted, or underweight (de Onis, Monteiro, Akre et al. 1993). It is probable that many of them also suffer from VADD, but statistics are not available because in recent years the terms PEM, kwashiorkor and marasmus for the severe clinical forms of childhood malnutrition have been abandoned and there are no records of their prevalence, trends, or mortality worldwide.
Another important feature of the setting of VADD is the frequency of the infectious diseases that accompany them. The relationship is synergistic: VAD weakens the defenses of the body and has specific damaging effects on the immune response (see Chapter 6). Infections in turn often impair vitamin A status by decreasing appetite, increasing demands on the body, and sometimes causing loss of the vitamin through the urine (see Chapter 14).
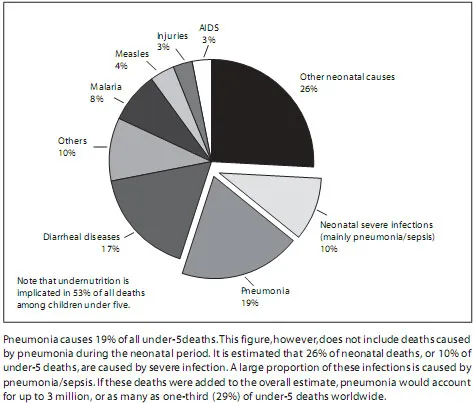
Recent estimates by WHO (Bryce, Boschi-Pinto, Shibuya et al. 2005) suggest that approximately 10.6 million children under the age of five die annually, most in developing countries. In the same report, pneumonia, surprisingly, turned out to be the leading killer of children, responsible for about one third of all deaths under five (fig. 1.1).
Undernutrition was an underlying cause in 53% of all deaths presented here. Further details are not available, but it would be reasonable to assume, from work referred to below (see Bryce, Black, Walker et al. 2005), that VAD and zinc deficiency play an important role. However, it appears that the term ‘undernutrition’ only applies to the presence of wasting and/or stunting. Growth retardation is associated with deficiencies of vitamin A or zinc, and possibly with other micronutrient deficiencies. In 2002 a groundbreaking study was published which showed the global and regional burden of disease and the 26 selected major risk factors responsible (Ezzati, Lopez, Rodgers et al. 2002). The burden of disease was measured as death and disability, represented by a unit termed ‘disability-adjusted life year’ (DALYs). Child and maternal underweight were the fourth highest cause of mortality, with high blood pressure as the first. When deficiency of iron, zinc and vitamin A are added to underweight, to form a category of malnutrition of their own, the outcome is then second overall. For DALYs, undernutrition is the single leading global cause of loss of health constituting 16% of the total burden. For iron, vitamin A, and zinc deficiency, the DALYs are 2.4%, 1.8%, and 1.9%, with iodine deficiency only 0.1%.
Fig. 1.1. Pneumonia is the leading killer of children worldwide. This figure shows global distribution of cause-specific mortality among children under five in 2004 (Bryce, Boschi-Pinto, Shibuya et al.2005).
In 2006 (Lopez, Mathers, Ezzati et al.) an update of these data showed some changes. Child underweight for age became the fourth attributable cause of deaths, with zinc, vitamin A, and iron deficiencies in 12th, 14th and 15th positions respectively. For the attributable disease burden (% global DALYs), child underweight for age was first, with zinc, iron, and vitamin A deficiencies 11th, 13th and 14th respectively. In the first of a series of papers, known as The Lancet Series, devoted to the latest assessment of ‘Maternal and child malnutrition’, Black, Allen, Bhutta et al. (2008) dealt with global and regional exposures and health consequences. It was estimated that ...