![]()
Koletzko B, Poindexter B, Uauy R (eds): Nutritional Care of Preterm Infants: Scientific Basis and Practical Guidelines.
World Rev Nutr Diet. Basel, Karger, 2014, vol 110, pp 99-120 (DOI: 10.1159/000358461)
______________________
Water, Sodium, Potassium and Chloride
Christoph Fuscha · Frank Jochumb
aDepartment of Pediatrics, McMaster University & Hamilton Health Sciences, Hamilton, Ont., Canada; bDepartment of Pediatrics, Evangelisches Waldkrankenhaus Spandau, Berlin, Germany
Reviewed by Brenda Poindexter, Riley Hospital for Children at Indiana University Health, Indianapolis, Ind., USA; Ricardo Uauy, National Institute of Nutrition and Food Technology, University of Chile, Santiago de Chile, Chile
______________________
Abstract
The sudden disruption of excessive placental supply with fluids and electrolytes is challenging for neonatal physiology during the period of postnatal adaptation. Different from many other nutrients, the body experiences large changes in daily requirements during the first 7-14 postnatal days, and on the other hand does not tolerate conditions of excess and deficiency very well. Imbalances of fluid and electrolytes are common in neonates, which – in addition – might be further aggravated by NICU treatment procedures. Therefore, fluid and electrolyte management can be one of the most challenging aspects of neonatal care of the premature infant. An understanding of the physiological adaptation process to extrauterine life – and how immaturity effects that transition – is the basis which is needed to understand and manage fluid and electrolyte balance in premature infants. This chapter addresses the physiology of postnatal adaptation and other aspects of fluid and electrolyte management (concerning potassium, sodium and chloride) of the preterm infant.
© 2014 S. Karger AG, Basel
'Water – the major nutrient' is the title of a review published in 1982 by Bent Friis-Hansen in the Journal of Pediatrics [1]. This title illustrates that water represents the major component of the human body as well as of enteral and parenteral nutrition [2]. The homeostasis of a mammalian organism depends on intact water metabolism. Water is integral to all of life's functions. It carries nutrients to cells, removes waste, and makes up the physicochemical milieu that allows cellular work to occur. Different from most nutrients, the human body has no water stores and needs a continuous 'short interval' supply to assure basal metabolic processes.
Water physiology and homeostasis show the highest inter- and intraindividual variation when compared to all other nutrients. This is caused by individual differences in body size, proportion, body surface, skin properties as well as conditions occurring during the period of postnatal transition in relation to immaturity, postnatal age and intensity of support needed.
Physiology
Knowledge about the physiology of water and electrolyte metabolism is needed for safe administration of fluids and electrolytes, and to become competent to adjust these to actual needs of a newborn in order to avoid harm. Too low intake may compromise circulation and metabolism, while inappropriate high intake of fluid or electrolytes may lead to or promote conditions like patent ductus arteriosus (PDA), chronic lung disease (CLD), etc.
Water is not equally distributed within the different body compartments. Fat mass is the energy store of the body and shows the highest inter- and intraindividual variability of all body compartments. Energy metabolism occurs only in the cytoplasma of the adipocyte, mostly to maintain intracellular homeostasis, to store and release triglycerides as well as to produce hormones like leptin. The major part of the adipocyte is the triglyceride-containing vacuole which is assumed to be free of water.
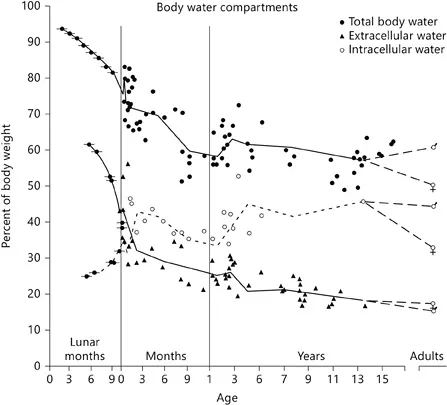
Lean mass represents a metabolically active cell mass. It consumes most of the body's energy by substrate oxidation and protein synthesis. Water is found only in lean tissue, thus metabolism of water and electrolytes is correlated closer with lean than with total body mass – of importance when subjects with different body composition are compared. Body water decreases remarkably during early life – from 90% at 24 gestational weeks to 75% at term [3, 4], mostly because fat mass is accumulated during the third trimester [5]. The time course of the water content of the human body during the entire lifespan is given in figure 1.
Body Water Compartments
Within lean mass body water is separated in different compartments, each playing a different physiological role and experiencing different physiological conditions and regulatory mechanisms.
Intracellular Fluid (ICF) and Extracellular Fluid (ECF): The ICF is located within the cytoplasm, enveloped by the double-lipid cellular membrane. Its leading ion is potassium. ECF represents water volume outside the cell membrane. Its leading ion is sodium. ECF is subdivided into intravascular (IVC) and extravascular (EVC) compartments as well as a 'third space' which characterizes free fluid in preformed cavities under physiological (e.g. urine, CSF) and pathological conditions (e.g. ascites, pleural effusions). ECF and IVC decrease during childhood. In preterm and term infants, total blood volume is 85-100 ml/kg compared to 60-70 ml/kg in adults [6-8].
The sizes of water compartments in healthy term infants on day 1 of life are (% of body weight) 75 ± 5% for body water, 31 ± 6% for ECF, 44 ± 8% for ICF and 10 ± 1% for IVC [9]. In ELBW infants ECF is 48 ± 11% [10].
Fig. 1. Age-related changes of total body water and its compartments, the intracellular and extracellular volume, from fetal life until adolescence [2].
Mechanisms That Regulate Body Fluids (fig. 2)
Control of Body Water: Whole-body water homeostasis is regulated via ECF, it serves as an interface with the environment. ECF regulation (intake, absorption, excretion) is effected via IVC volume. The amount of water and sodium is independently regulated – within certain limits. The regulatory response must (1) maintain adequate circulation and blood pressure and (2) keep osmolality of the ECF compartment within 3% of the set point (280-290 mosm) [11-13]. Regulation is achieved through changes in intake via (i) thirst (except for newborns when intake is controlled by others), (ii) vascular tone, heart rate and contractility, and (iii) renal excretion of water and electrolytes. The system is modulated through hormonal action on renal excretion of water and solutes, including the renin-angiotensin-aldosterone system, arginine vasopressin, and atrial natriuretic peptide.
The ECF control mechanism functions as follows: ECF increase leads to an increase in IVC volume and blood pressure. Increased vascular pressure increases urinary flow until the ECF volume returns to baseline. Hypotonicity suppresses antidiuretic hormone secretion, thus diluting urinary osmotic load [13, 14]. Conversely, a decrease in ECF volume results in decreased cardiac output and glomerular filtration pressure, leading to decreased urinary flow that lasts until intake replenishes the lost volume. Hypertonicity, which accompanies many low-volume states, stimulates thirst and renal resorption of water [15].
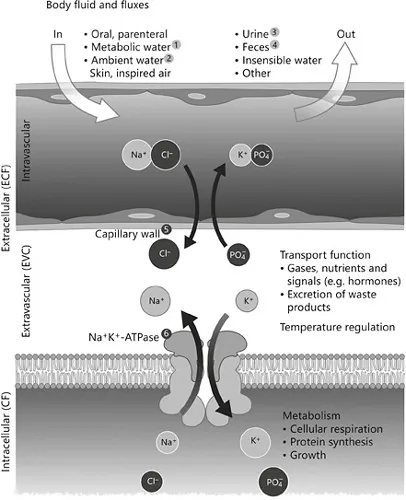
Fig. 2. Water and electrolyte fluxes between body water compartments. Remarks: 1) metabolic water production depending on exact intake of carbohydrates, protein and fat(approx. 15 ml/kg/day), 2) input via skin and inspired air (see fig. 3), 3) volume depending upon need for excretion of fixed acids and urea and desired urine osmolarity, 4) fecal water losses: quantities are negligibly small in healthy subjects, but considerable in diarrhea and/or in presence of ileostoma (e.g. NEC surgery), 5) oncotic pressure, 6) activity of Na+/K+-ATPase defines the long-term ratio of ECF/ICF; short-term changes are subject to short-term variation of ECV; content of water and electro-/osmolytes: any change in either ICV or ECV osmolarity will result in movement of water into the compartment with the higher osmolarity.
Regulation of ICF and ECF: The different electrolyte concentrations of ICF and ECF are achieved by energy-dependent active transport of Na+/K+-ATPase. It also establishes the transmembranal Na+/K+ gradient by continuously shuffling Na+ ions out of, and K+ ions into the cell. Cellular membranes thus appear to be relatively impermeable to sodium. The Na+/K+-ATPase pump is the most important regulator of the ICF:ECF ratio [16, 17]. As a consequence, ICF is shielded from direct interface with the external environment preventing most tissues from sudden and large changes of solute or water concentration. Studies in endothelial cells show that Na+/K+-ATPase consumes abou...