
eBook - ePub
Glaucoma
C. E. Traverso, I. Stalmans, F. Topouzis, L. Bagnasco
This is a test
Partager le livre
- 130 pages
- English
- ePUB (adapté aux mobiles)
- Disponible sur iOS et Android
eBook - ePub
Glaucoma
C. E. Traverso, I. Stalmans, F. Topouzis, L. Bagnasco
Détails du livre
Aperçu du livre
Table des matières
Citations
À propos de ce livre
Promising developments in the diagnosis and treatment of glaucoma are giving hope to millions of patients threatened by blindness worldwide. This 8th volume of the 'ESASO Course Series' is a manual containing the lectures from the ESASO glaucoma session held in 2016. Topics range from diagnostic techniques to therapies such as laser treatment, canaloplasty, and phacoemulsification. Antiscarring measures and the risk of glaucoma-related handicap are discussed. The contributors are renowned experts in the field of ophthalmology and the subspecialty of glaucoma. This easy-to-read text is intended to help solve practical clinical problems. Residents and established ophthalmologists will find it to be a beneficial source of current information.
Foire aux questions
Comment puis-je résilier mon abonnement ?
Il vous suffit de vous rendre dans la section compte dans paramètres et de cliquer sur « Résilier l’abonnement ». C’est aussi simple que cela ! Une fois que vous aurez résilié votre abonnement, il restera actif pour le reste de la période pour laquelle vous avez payé. Découvrez-en plus ici.
Puis-je / comment puis-je télécharger des livres ?
Pour le moment, tous nos livres en format ePub adaptés aux mobiles peuvent être téléchargés via l’application. La plupart de nos PDF sont également disponibles en téléchargement et les autres seront téléchargeables très prochainement. Découvrez-en plus ici.
Quelle est la différence entre les formules tarifaires ?
Les deux abonnements vous donnent un accès complet à la bibliothèque et à toutes les fonctionnalités de Perlego. Les seules différences sont les tarifs ainsi que la période d’abonnement : avec l’abonnement annuel, vous économiserez environ 30 % par rapport à 12 mois d’abonnement mensuel.
Qu’est-ce que Perlego ?
Nous sommes un service d’abonnement à des ouvrages universitaires en ligne, où vous pouvez accéder à toute une bibliothèque pour un prix inférieur à celui d’un seul livre par mois. Avec plus d’un million de livres sur plus de 1 000 sujets, nous avons ce qu’il vous faut ! Découvrez-en plus ici.
Prenez-vous en charge la synthèse vocale ?
Recherchez le symbole Écouter sur votre prochain livre pour voir si vous pouvez l’écouter. L’outil Écouter lit le texte à haute voix pour vous, en surlignant le passage qui est en cours de lecture. Vous pouvez le mettre sur pause, l’accélérer ou le ralentir. Découvrez-en plus ici.
Est-ce que Glaucoma est un PDF/ePUB en ligne ?
Oui, vous pouvez accéder à Glaucoma par C. E. Traverso, I. Stalmans, F. Topouzis, L. Bagnasco en format PDF et/ou ePUB ainsi qu’à d’autres livres populaires dans Medicine et Public Health, Administration & Care. Nous disposons de plus d’un million d’ouvrages à découvrir dans notre catalogue.
Informations
Sujet
MedicineSous-sujet
Public Health, Administration & CareTraverso CE, Stalmans I, Topouzis F, Bagnasco L (eds): Glaucoma.
ESASO Course Series. Basel, Karger, 2016, vol 8, pp 52-75 (DOI: 10.1159/000446142)
ESASO Course Series. Basel, Karger, 2016, vol 8, pp 52-75 (DOI: 10.1159/000446142)
______________________
Treatment of Glaucoma with or without Medications Lowering Intraocular Pressure: Options and Relevant General Health Issues
John Thygesen
Department of Ophthalmology, Rigshospitalet, Copenhagen University Hospital, Glostrup, Denmark
______________________
Abstract
The etiology of glaucoma is multifactorial. Intraocular pressure (IOP) is the only modifiable factor in glaucoma management proven to alter the natural course of the disease. Currently, based on evidence-based glaucoma therapy, the only approach proven to be efficient in preserving visual function is lowering IOP. Lowering IOP by 20-40% has been shown to reduce the rate of progressive visual field loss by half. Despite the fact that IOP-lowering interventions reduce the risk of progression and delay the onset of glaucoma, its pathogenesis is controversial and not completely understood. In this matter, non-IOP-dependent risk factors appear to be responsible for around 50% of glaucoma cases. New drugs are now entering the clinic, along with new ways to deliver them. There is growing consensus that the future of glaucoma management will be based more on the optic nerve pathway from the retina to the visual cortex and will not be strictly limited to improving outflow or reducing inflow. But still, many future IOP-lowering options will be developed, including neuroprotective strategies aiming to directly prevent or significantly hinder neuronal cell damage. The goal of glaucoma treatment is to maintain the patient’s visual function and related quality of life at a sustainable cost. The cost of treatment in terms of inconvenience and side effects as well as financial implications for the individual and society requires careful evaluation. In conclusion, IOP lowering is the only proven therapy for glaucoma at present. Neuroprotection may be clinically useful (based on one trial), but this needs to be confirmed. So far, we have no evidence of potential therapies related to ocular blood flow and glaucoma care, and evidence to support the use of acupuncture, vitamins, minerals, or herbal medicines such as marijuana for treating glaucoma is insufficient.
© 2016 S. Karger AG, Basel
Introduction
The first part of the chapter is based upon the European Glaucoma Society (EGS) Guidelines 2014 (www.eugs.org).
Glaucoma refers to a group of eye conditions that cause chronic, progressive optic neuropathies with common morphological changes at the optic nerve head (ONH) and the retinal nerve fiber layer. These changes are associated with progressive retinal ganglion cell (RGC) death that may lead to characteristic damage to the visual field.
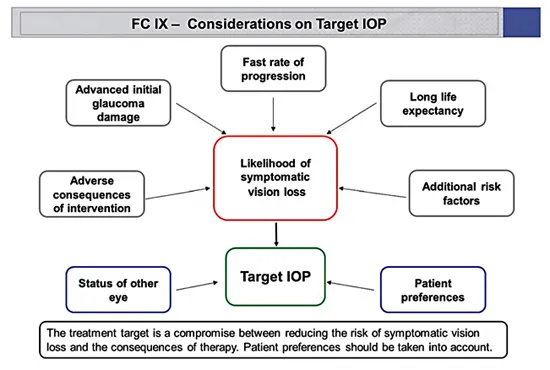
Fig. 1. Considerations on target IOP. Reprinted with permission from the European Glaucoma Society (EGS Guidelines 2014).
The most common subtype of glaucoma is primary open-angle glaucoma (POAG). Despite the normal clinical appearance of the drainage pathway, the aqueous outflow is restricted in most POAG cases. The increased intraocular pressure (IOP) that may follow is referred to as the main risk factor for glaucoma progression.
Glaucoma Therapy
Lowering Intraocular Pressure
Evidence-Based Glaucoma Therapy: Still to Lower Intraocular Pressure
The etiology of glaucoma is multifactorial. IOP is the only modifiable factor in glaucoma management proven to alter the natural course of the disease. Lowering IOP by 20-40% has been shown to reduce the rate of progressive visual field loss by half [1, 2]. Currently, the only approach proven to be efficient in preserving visual function is lowering IOP [3-5].
Despite the fact that IOP-lowering interventions reduce the risk of progression and delay the disease onset of glaucoma, its pathogenesis is controversial and not completely understood. In this matter, non-IOP-dependent risk factors appear to be responsible for around 50% of glaucoma cases [6].
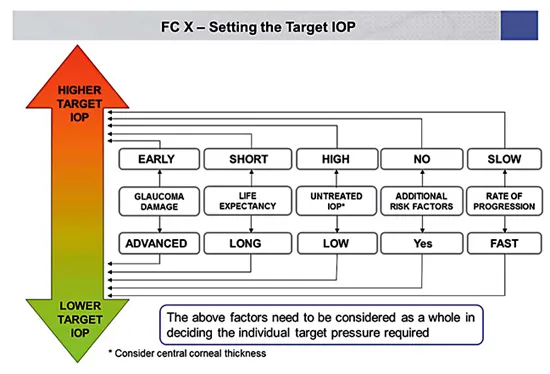
Fig. 2. Setting the target IOP. Reprinted with permission from the European Glaucoma Society (EGS Guidelines 2014).
Perfusion Pressure
Other possible treatment areas have been investigated, including ocular blood flow and neuroprotection. There are experimental as well population-based studies indicating that perfusion pressure may be relevant in glaucoma [7-10] but very difficult to measure. An increase in IOP will lead to a reduction in perfusion pressure. Blood pressure levels may also be important in glaucoma. However, there is no conclusive evidence to support the idea that perfusion pressure can be increased by manipulating blood pressure or ocular blood flow in glaucoma patients.
Neuroprotection
Neuroprotection can be defined as a ‘therapeutic approach’ aiming to directly prevent, hinder, and, in some cases, reverse neuronal cell damage. Since glaucoma can continue deteriorating in spite of an apparently well-controlled IOP, the need for effective non-IOP-related treatments is widely acknowledged. Several compounds have been shown to be neuroprotective in animal models of experimental glaucoma. So far, no compound has reached a sufficient level of evidence to be considered as a neuroprotectant in humans. A large long-term randomized trial using a neuroprotective agent, memantine, was analyzed several years ago, but with negative results. A more recent study claiming that topical brimonidine might have neuroprotective properties in glaucoma patients has been questioned in a systematic review on neuroprotection in glaucoma [11, 12].
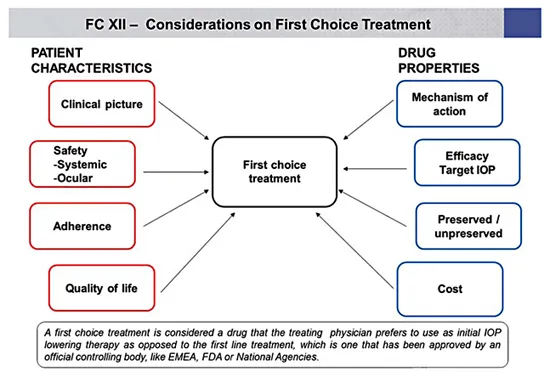
Fig. 3. Considerations on first-choice treatment. Reprinted with permission from the European Glaucoma Society (EGS Guidelines 2014).
Target Intraocular Pressure
Therapy in glaucoma management aims to lower IOP to slow the rate of visual field deterioration.
Target IOP is the upper limit of the IOP estimated to be compatible with a rate of progression sufficiently slow to maintain vision-related quality of life in the expected lifetime of the patient. It should be reevaluated regularly and, additionally, when progression of disease is identified or when ocular or systemic comorbidities develop.
There is no single target IOP level that is appropriate for every patient, so the target IOP needs to be estimated separately for each eye of every patient (fig. 1-3).
Antiglaucoma Drugs
Several prospective randomized multicenter controlled clinical studies have clearly established the benefits of IOP reduction in managing POAG at various stages of the disease whether of the ‘high-pressure’ or ‘normal-pressure’ variety as well as reducing the conversion of ocular hypertension to POAG [13-17].
Most forms of open-angle glaucoma and many types of chronic angle closure glaucoma are initially treated with topical and occasionally orally administrated agents that act either on the reduction of aqueous humor production or enhancement of the aqueous outflow, or on both. Although acute angle closure with or without glaucoma needs rapid laser or incisional surgery, medical treatment will usually be initiated as a first step in most cases.
Laser treatment may be a suitable first option for patients with known intolerance or allergy to topical agents, or suspected poor compliance.
When initially selecting medical therapy it is important to cons...