![]()
Lloyd SKW, Donnelly NP (eds): Advances in Hearing Rehabilitation.
Adv Otorhinolaryngol. Basel, Karger, 2018, vol 81, pp 93–104 (DOI: 10.1159/000485526)
______________________
Hearing Rehabilitation in Neurofibromatosis Type 2
Hannah J.D. Northa · Simon K.W. Lloydb
aWestmead Hospital, Sydney, NSW, Australia; bUniversity Department of Otolaryngology Head and Neck Surgery, Peter Mount House, Manchester Royal Infirmary, Manchester, UK
______________________
Abstract
Bilateral vestibular schwannomas are almost pathognomonic of neurofibromatosis type 2 (NF2). As a result of these tumors, hearing loss is the presenting symptom in 60% of adults and 30% of children with NF2. It is often bilateral. The best means of preserving hearing in patients with NF2 is conservative management. Even so at least 28% of patients have progression of hearing loss following diagnosis. The likelihood of progression of hearing loss is, at least in part, determined by the type of mutation. Treatment of vestibular schwannomas often has a detrimental effect on hearing. Only 41% of patients having stereotactic radiosurgery maintain their hearing at 5 years. Treatment with bevacizumab maintains medium-term hearing in 38% and improves it in 48%. Surgery to remove vestibular schwannomas invariably leads to complete loss of ipsilateral hearing, although in a very limited number of patients hearing preservation surgery may be possible. For those that lose their hearing but have an intact cochlear nerve, for example, conservative management, radiotherapy treatment or cochlear nerve preserving surgery, cochlear implantation has been shown to be an effective option although outcomes are not as good as traditional implant candidates (mean sentence testing scores in quiet: stable untreated tumors 69%; radiotherapy treated tumors 49%; cochlear nerve preserving surgery ∼40%). For those that do not have a functional cochlear nerve, auditory brainstem implantation (ABI) is an option. The non-user rate in this group is 13%. The mean sentence score in users with ABI alone is 12%. ABI therefore acts, in most cases, as an aid to lip reading and rarely provides open set speech discrimination.
© 2018 S. Karger AG, Basel
Introduction
Hearing loss is one of the main factors influencing the quality of life in patients with neurofibromatosis type 2 (NF2) [1–3]. It is almost inevitable either as a result of the presence of bilateral vestibular schwannoma or its treatment. Its effects are more devastating in NF2 compared to those with sporadic unilateral vestibular schwannomas because of the hearing loss is often bilateral rather than unilateral.
Decision making around hearing preservation or rehabilitation in patients with NF2 is complex. It must be balanced with the need for tumor control in the presence of an often aggressive disease and with the potential risk of a given intervention. This is made more complicated by the fact that both ears must be taken into consideration.
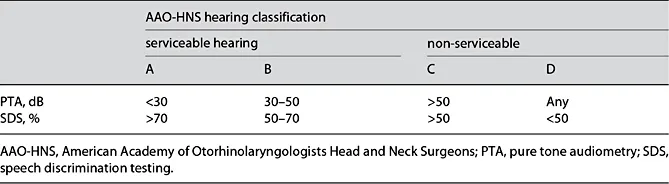
Table 1. AAO-HNS categories of hearing loss
Table 2. UK NF2 consensus group grading system for the assessment of hearing loss in NF2
Grade | Test | Deficit |
1 | >70% SDS in better hearing ear | Normal or near normal hearing with or without acoustic hearing aids |
2 | 50–69% SDS in better hearing ear | Good benefit from acoustic hearing aids |
3 | <50% SDS in better hearing ear; ≥50% BKB | Adequate benefit from acoustic hearing aids, best-aided condition |
4 | <50%SDS in better hearing ear; <50% BKB | Poor benefit from acoustic hearing aids, consider auditory implant |
5 | Auditory implant | |
6 | Dead ear | |
Speech discrimination score (SDS) is the percentage of phonemes within 10 monosyllabic words correctly identified at an optimal sound intensity. Bamford-Kowal-Bench (BKB) standard sentence lists comprise 21 lists, each having 16 sentences and 50 keywords (3 or 4 per sentence) presented at an optimal sound intensity. |
In the past 25 years, the hearing rehabilitation options available to clinicians have expanded considerably, particularly with the introduction of less invasive treatments such as chemotherapy and the availability of electrical stimulation of the cochlear nerve with cochlear implantation and of the cochlear nucleus with auditory brainstem implantation (ABI).
The following chapter summarizes the current evidence base behind the management options available to patients with NF2.
The Natural History of Hearing in NF2
Outcome Measurements of Hearing Loss
Most clinicians use the American Academy of Otorhinolaryngologists Head and Neck Surgeons (AAO-HNS) hearing classification system to categorize the severity of hearing loss (Table 1). This in turn can determine the hearing rehabilitation recommendations. A consensus document on the evaluation of hearing loss in NF2 has been published by the UK NF2 group (Table 2) [4]. In the UK, it is recommended that patients with NF2 should have an annual pure tone audiometry and speech discrimination testing (SDS) with Arthur Bothroyd words. If required, annual hearing aid assessments are also undertaken to ensure hearing is optimized. Once SDS is <50%, annual Bamford-Kowal-Bench (BKB) sentence testing is undertaken. This should be performed in best aided conditions and with optimum sound intensity, as determined by the SDS. BKB sentence scores of <50% indicate that the patient is struggling with conventional hearing aids and should then be assessed for auditory implantation. Plotkin et al. [5] have put forward a consensus statement on reporting hearing and tumor treatment outcomes in patients with NF2 (Table 3).
Table 3. Minimum documentation recommended in patients with NF2
For all cases Mean tumor size at treatment (this should be recorded according to CPA component and, where possible as a volume in cm3) Annual tumor growth Mean tumor size at last follow-up, if relevant Completeness of tumor removal, if relevant Radiological recurrence rate, if relevant Duration of follow-up (this should ideally be at least 5 years) |
For hearing preservation interventions Pure tone and speech discrimination data prior to commencement of treatment and at last follow-up according to AAO-HNS recommendations. As well as SDS at 40 dB, the maximum SDS and the sound intensity at which it is achieved should also be recorded Proportion maintaining serviceable hearing (defined as AAO-HNS class A or B) Tumor control (this should be defined as no change in size within 2 mm of pre-treatment scan on imaging not as no intervention) For radiotherapy, technique used and marginal/maximum radiation dose |
For auditory implantation Speech discrimination scores with and without lip reading in quiet and in noise with sentences delivered at 70 dB For patients with poor outcomes, word scores and environmental sound awareness assessment Implant user Use of telephone |
It is important to note that, because of the bilateral nature of NF2 vestibular schwannomas, it is likely that class C or even good class D hearing will be helpful if the contralateral ear is profoundly deaf, and this should be taken into consideration when making management decisions that could potentially affect residual hearing.
Hearing at Presentation
Hearing loss in patients with NF2 is most commonly attributed to vestibular schwannomas, although it may result from cochlear schwannomas, cerebellopontine angle (CPA) meningiomas or middle ear dysfunction from middle fossa meningiomas. The degree of hearing loss at presentation varies in patients with vestibular schwannomas. Historically, hearing loss has been common at initial presentation, occurring in 60% of adults and 30% of children [6]. Surprisingly, more recent prospective studies show a large proportion of patients with no or minimal hearing loss at presentation. For example, Plotkin et al. [7] found that 71% of patients with NF2 have no hearing loss at presentation (AAO class A). It is probable that this difference relates to a higher proportion of patients being diagnosed early with milder phenotypes and smaller tumors as a result of improvements in imaging and screening protocols. When hearing loss is present at presentation, it is often unilateral. Peyre et al. [8] found that 85% of patients with NF2 had serviceable hearing in at least one ear at presentation.
Deterioration of Hearing
With time, hearing loss often progresses to a bilateral hearing loss, although this may remain asymmetrical [6]. This hearing loss may be gradual, stepwise or sudden, with between 5 and 15% having sudden hearing loss [9, 10]. In Plotkin’s patient group [5], 28% of patients experienced hearing decline (defined as an increase in threshold of >6 dB) over a median period of 62 months. Five percent had a hearing decline at 1 year, 13% had a hearing decline at 2 years and 16% had a hearing decline at 3 y...