
eBook - ePub
Bergman's Comprehensive Encyclopedia of Human Anatomic Variation
R. Shane Tubbs, Mohammadali M. Shoja, Marios Loukas, R. Shane Tubbs, Mohammadali M. Shoja, Marios Loukas
This is a test
Partager le livre
- English
- ePUB (adapté aux mobiles)
- Disponible sur iOS et Android
eBook - ePub
Bergman's Comprehensive Encyclopedia of Human Anatomic Variation
R. Shane Tubbs, Mohammadali M. Shoja, Marios Loukas, R. Shane Tubbs, Mohammadali M. Shoja, Marios Loukas
Détails du livre
Aperçu du livre
Table des matières
Citations
À propos de ce livre
Building on the strength of the previous two editions, Bergman's Comprehensive Encyclopedia of Human Anatomic Variation is the third installment of the classic human anatomical reference launched by Dr. Ronald Bergman. With both new and updated entries, and now illustrated in full color, the encyclopedia provides an even more comprehensive reference on human variation for anatomists, anthropologists, physicians, surgeons, medical personnel, and all students of anatomy.
Developed by a team of editors with extensive records publishing on both human variation and normal human anatomy, Bergman's Comprehensive Encyclopedia of Human Anatomic Variation is the long awaited update to this classic reference.
Foire aux questions
Comment puis-je résilier mon abonnement ?
Il vous suffit de vous rendre dans la section compte dans paramètres et de cliquer sur « Résilier l’abonnement ». C’est aussi simple que cela ! Une fois que vous aurez résilié votre abonnement, il restera actif pour le reste de la période pour laquelle vous avez payé. Découvrez-en plus ici.
Puis-je / comment puis-je télécharger des livres ?
Pour le moment, tous nos livres en format ePub adaptés aux mobiles peuvent être téléchargés via l’application. La plupart de nos PDF sont également disponibles en téléchargement et les autres seront téléchargeables très prochainement. Découvrez-en plus ici.
Quelle est la différence entre les formules tarifaires ?
Les deux abonnements vous donnent un accès complet à la bibliothèque et à toutes les fonctionnalités de Perlego. Les seules différences sont les tarifs ainsi que la période d’abonnement : avec l’abonnement annuel, vous économiserez environ 30 % par rapport à 12 mois d’abonnement mensuel.
Qu’est-ce que Perlego ?
Nous sommes un service d’abonnement à des ouvrages universitaires en ligne, où vous pouvez accéder à toute une bibliothèque pour un prix inférieur à celui d’un seul livre par mois. Avec plus d’un million de livres sur plus de 1 000 sujets, nous avons ce qu’il vous faut ! Découvrez-en plus ici.
Prenez-vous en charge la synthèse vocale ?
Recherchez le symbole Écouter sur votre prochain livre pour voir si vous pouvez l’écouter. L’outil Écouter lit le texte à haute voix pour vous, en surlignant le passage qui est en cours de lecture. Vous pouvez le mettre sur pause, l’accélérer ou le ralentir. Découvrez-en plus ici.
Est-ce que Bergman's Comprehensive Encyclopedia of Human Anatomic Variation est un PDF/ePUB en ligne ?
Oui, vous pouvez accéder à Bergman's Comprehensive Encyclopedia of Human Anatomic Variation par R. Shane Tubbs, Mohammadali M. Shoja, Marios Loukas, R. Shane Tubbs, Mohammadali M. Shoja, Marios Loukas en format PDF et/ou ePUB ainsi qu’à d’autres livres populaires dans Biological Sciences et Human Anatomy & Physiology. Nous disposons de plus d’un million d’ouvrages à découvrir dans notre catalogue.
Informations
1
Skull
Selcuk Tunali
TOBB University of Economics and Technology, Ankara, Turkey
University of Hawaii, Honolulu, Hawaii, United States
University of Hawaii, Honolulu, Hawaii, United States
Frontal bone
The frontal sinus ostium is sometimes absent. In a cadaveric study, Ozgursoy et al. (2010) reported absence of right frontal sinus ostium in 3.6% of cases when there was a connection between the right and left frontal sinuses. They also noted that if one of the frontal sinus ostia cannot be found during sinus surgery, although this sinus and its recess can be seen on thick-sliced coronal computed tomographic scans, there could be an agenetic frontal sinus hidden by the extensive pneumatization of the contralateral sinus that crosses the midline (3.6%).
The frontal sinus itself can be absent. Computed tomographic scans in the axial and coronal planes of the frontal sinuses of 565 patients were examined. There was bilateral agenesis of the frontal sinus in 8.32% of these cases and unilateral absence of the frontal sinus in 5.66% (Danesh-Sani et al. 2011).
Another study investigated the prevalence of agenesis of the frontal sinuses using dental volumetric tomography (DVT) in Turkish individuals. The frontal sinuses of 410 patients were examined by DVT scans in the coronal plane. There was bilateral and unilateral absence of the frontal sinuses in 0.73% and 1.22% of cases, respectively (Çakur et al. 2011aa). Aydinlioğlu et al. (2003) studied computed tomography (CT) scans of the paranasal sinuses in the axial and coronal planes from a series of 1200 cases. Bilateral and unilateral absences of the frontal sinuses were noted in 3.8% and 4.8%, respectively.
In a study on the septation of the frontal sinuses, Comer et al. (2013) concluded that frontal sinus septations appear to be significantly associated with and predictive of the presence of supraorbital ethmoid cells. Identifying frontal sinus septations on sinus CT could therefore imply a more complex anatomy of the frontal recess.
In a study by Bajwa et al. (2013), all patients older than 15 months and 23 days had completely fused metopic sutures. The estimated median age for the start of the fusion process was 4.96 months (95% confidence interval, 3.54–6.76 months), and the estimated median age for completion of fusion was 8.24 months (95% confidence interval, 7.37–9.22 months). The fusion process was complete between 2.05 and 14.43 months of age in 95% of the normal population. There was no significant difference between sexes. This study demonstrated wide variation in the timing of normal fusion, which can complete as early as two months of age (Bajwa et al. 2013).
Persistent metopic sutures can be misdiagnosed as vertical traumatic skull fractures extending down the midline in head trauma patients. The surgeon should therefore be aware of this anatomical variant during primary and secondary surveillance of the traumatized patient and during surgical intervention, especially including frontal craniotomy. A reconstructed tomography scan demonstrating sutural closuring status could provide useful additional information in the diagnostic sequence, superior to a plain X-ray in the emergency setting (Bademci et al. 2007). Nakatani et al. (1998) encountered a complete ectometopic suture in a 91-year-old Japanese male cadaver during a gross anatomy course. It was observed in 1 of 26 skulls aged 62–92 years and was about 13 cm long from the bregma to the nasion. A metopic suture is rare in a person of advanced age, as in their case.
In another study, 1276 adult Indian skulls were examined for the incidence of metopic sutures. There was metopism in 2.66% of the skulls and metopic sutures were present in 38.17% (35.27% in the lower part of the frontal bone in various shapes); the incidences in the upper, upper middle and lower middle parts of the frontal bone were 0.8% in each location. As well as the abovementioned findings, a peculiar shape (inverted Y) was seen in 0.63% and a radiating type in 0.31% of the skulls (Agarwal et al. 1979).
Hyperostosis frontalis interna is a condition of bony overgrowth of the frontal region of the endocranial surface, appearing in the scientific literature as early as 1719. During routine dissection of a donor’s calvaria it was noted that she had significant bony overgrowth of the endocranium. Such overgrowth was diffuse throughout the frontal bone, extending slightly into the parietal region with midline sparing (Fig. 1.1). It ranged from 1.0 cm thickness in the temporal region to 1.3 cm adjacent to the midline in the frontal region. Large individual nodules were located along either side of the frontal crest at the intersection of the frontal and parietal bones. The largest nodules measured 2.08 cm in thickness on the right and 1.81 cm on the left (Fig. 1.2). As a result, the pathway of the middle meningeal artery was tortuous. In addition there was significant bilateral depression of the frontal lobes and surrounding neural tissues (Fig. 1.3) (Champion and Cope 2012).
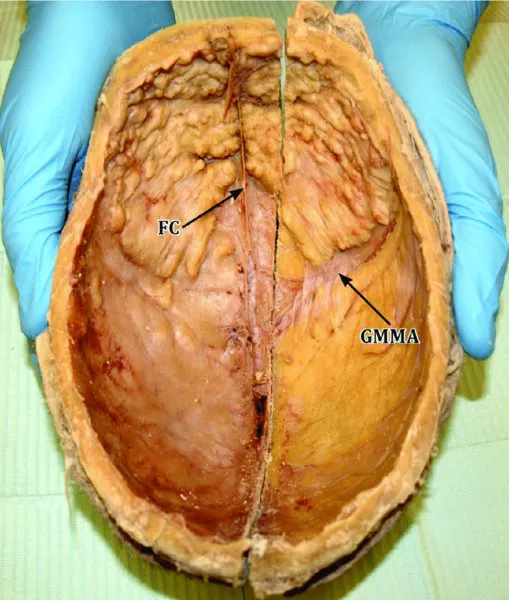
Figure 1.1 Severe case of hyperostosis frontalis interna with typical midline sparing along the frontal crest. Notice the tortuous pathway of the middle meningeal artery. FC: frontal crest; GMMA: groove for middle meningeal artery.
Source: Champion and Cope (2012). Reproduced with permission from International Journal of Anatomical Variations.
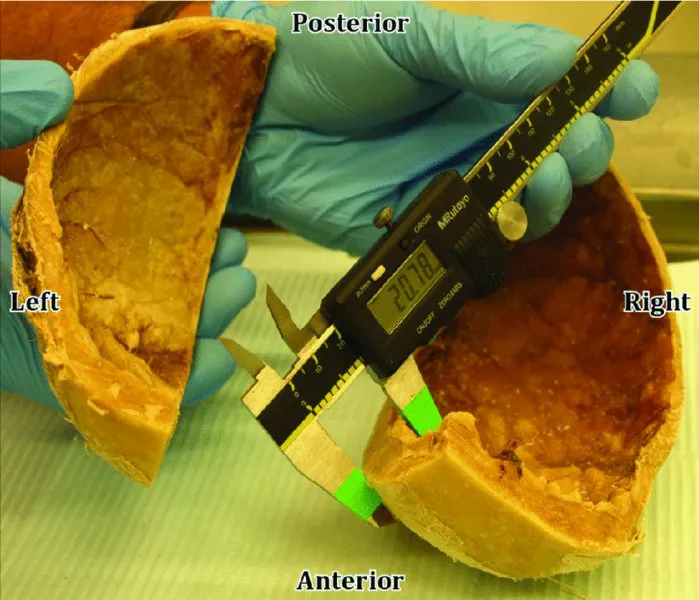
Figure 1.2 Picture shows the measurement of a large nodule (2.08 cm) located adjacent to the frontal crest at the juncture of the frontal and parietal bones.
Source: Champion and Cope (2012). Reproduced with permission from International Journal of Anatomical Variations.
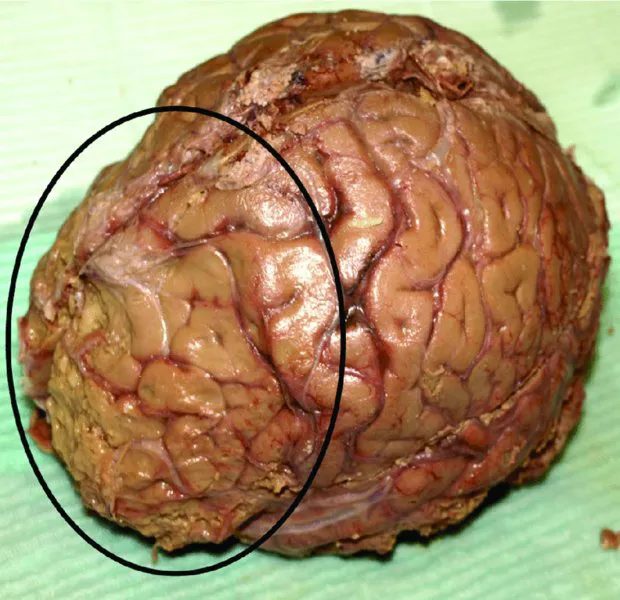
Figure 1.3 Notice the significant compression of the frontal lobes.
Source: Champion and Cope (2012). Reproduced with permission from International Journal of Anatomical Variations.
Nikolić et al. (2010) determined the rate of occurrence and appearance of hyperostosis frontalis interna (HFI) in females and correlated this phenomenon with aging. The sample included 248 deceased females, 45 with different types of HFI and 203 without HFI, average ages 68.3±15.4 (range 19–93) and 58.2±20.2 years (range 10–101), respectively. The rate of HFI was 18.14%. The older the woman, the higher the possibility of HFI (Pearson correlation 0.211, N=248, P=0.001), but the type of HFI did not correlate with age (Pearson correlation 0.229, N=45, P=0.131). The frontal and temporal bones were significantly thicker in women with HFI than in women without it (t=–10.490, DF=246, P=0.000, and t=–5.658, DF=246, P=0.000, respectively). These bones became thicker with aging (Pearson correlation 0.178, N=248, P=0.005 and 0.303, N=248, P=0.000, respectively). The best predictors of HFI were frontal bone thickness, temporal bone thickness, and age (respectively: Wald coefficient=35.487, P=0.000; Wald coefficient=3.288, P=0.070, and Wald coefficient=2.727, P=0.099). Diagnosis of HFI depends not only on frontal bone thickness but also on the waviness of the internal plate of the frontal bone and the involvement of the inner bone surface (Nikolić et al. 2010). May et al. (2011) studied two female populations separated by a period of 100 years: 992 historical and 568 present-day females. HFI was detected by direct observation or CT images. HFI was significantly more prevalent in the present-day than the historical females (P<0....