![]()
The Development of a Fee Structure for Productivity Analysis and Program Management
Marilyn Dennis,MPA,OTR
Lana Ledet,OTR
SUMMARY. Occupational therapists are frequently promoted to management level positions without prior instruction in financial accounting. Accounting information can enhance rational decision making processes at both the middle management and supervisory levels. Although today's literature encourages health care professionals to utilize accounting principles, the occupational therapy manager is often uncertain as to how to apply these techniques to his own setting.
This paper describes how one multiclinic department revised its existing fee structure and utilized the generated data to analyze ther-apists' productivity and to effect decisions regarding program management.
OVERVIEW
A large occupational therapy department had a change of directors and other significant personal within a six month period. The director was confronted with the problem of reducing costs, while maintaining quality of care, enhancing productivity and developing a more judicious distribution of the 44 therapists and their assignments in a multiclinic department. This paper will describe the events related to the implementation of a relative value unit system for determining fees and staff productivity, an analysis of the data generated, and a description of how the outcomes of the productivity analyses were used for program decision making.
THE PARTICIPANTS
The primary author had just joined the department to supervise the physical dysfunction section. Because of her graduate training in public administration, and some previous experience in evaluating productivity in a smaller department, she was asked to develop a comprehensive charge system. The second author, meanwhile, had begun to develop skills in computer use. The two therapists combined efforts to develop a new charge system and a computer program to analyze the data generated by 44 therapists.
THE ORGANIZATION
The occupational therapy department is housed in a state medical university. The department director reports to an executive director for professional services of the university hospital. Occupational therapy is relatively autonomous in decision making. There are two assistant directors administering two distinct divisions: one in the physical dysfunction area, and the second in psychiatry and pediatrics. A leveling system provides recognition of staff's administrative and or clinical expertise; staff members may be designated as I, II, or Ill's contingent upon responsibilities and qualifications. Twelve occupational therapy clinics are geographically scattered throughout the 64 acre campus.
CHRONOLOGY OF EVENTS
In September of 1985, the director of occupational therapy expressed an interest in revising the existing fee structure and improving upon the means then available for therapists to document productivity. There were three essential functions involved in the process. The first consisted of revising the charge system based on data compilation, financial and staff accountability. The second function required data manipulation and analysis through the use of computer technology. The third and final function is an ongoing process requiring those in administration to make decisions based on the data which is compiled and analyzed monthly.
CONTEXT
Upon reviewing the existing charge mechanism, it was intended that the new system address several issues:
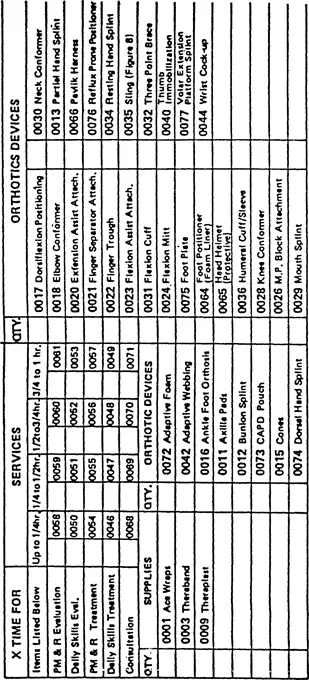
1. Charge categories that more appropriately described services rendered were needed to improve the department's ability to recover costs. The existing system listed only five service categories in which to describe treatment given. Treatment time could be charged in one quarter hour up to one hour units but time in excess of that was not being charged (Figure 1).
2. No means existed to differentiate the charges for a simple versus a complex treatment and/or evaluation. For example, a treatment in reality orientation would be billed under Physical Medicine and Rehabilitation at the same charge per time unit as a neuromuscular treatment. Reality orientation can often be performed by a COTA while a neuromuscular treatment may require the expertise of a therapist certified in NDT.
3. Uniform description of charge categories, adaptive equipment, and splints was also necessary to increase potential for third party payor reimbursement.
4. A procedure to allow therapists to charge for adaptive equipment lprovided to patients was critical. The existing structure did not offer this and equipment items were given to patients with no means of recovering costs to the department.
5. Reimbursement for occupational therapy services offered in psychiatry was a primary concern. The existing system did not allow for patient charges to be generated from that service area although one third of the occupational therapy staff were employed in this clinical area.
6. Group treatment charges were unavailable with the existing charge structure. The majoriity of psychiatric treatments were conducted in groups and thus required a lower fee per patient.
7. A more accurate reporting system for individual therapists, teams, and divisions to assess billable time was essential. This specific information would assist in determining plans for program development and more efficient assignment of personnel to teams. It would also increase administration's awareness of frequency of services rendered according to type of treatment, i.e., homemaking, neuromuscular; and group versus individual treatment as it related to various OTRs, COTAs, teams, and divisions.
Although the department is in a teaching hospital setting, and there are many demands on therapists beyond patient treatment (i.e., administrative tasks, clinic teaching, research and program development), therapists had not reached an adequate level of billable productivity (therapist time which can be charged to the patient, i.e., treatment preparation, direct patient care, documentation, travel time, and chart review). With the existing fee structure, departmental expenses were not being met. Also, the staff average daily treatment units did not match that of comparable departments elsewhere.
An unfortunate clinical reality is that however important some functions might be, not all of the therapist's functions are billable In this particular department, nonbillable or indirect patient care tasks had consisted of: performance of administrative tasks, student supervision, nonchargeable patient related activities such as scheduling, ordering equipment for the patient, and discussing patient's status informally with other disciplines, developing new programs,
EXISTING CHARGE SLIP — 1984
providing assistance to another therapist during patient treatment, and transportation of patients to and from clinics due to lack of an aide. It was apparent to administration that not only were these functions valid and deserving of recognition, but several tasks displayed reimbursement potential as well, i.e., ordering equipment for patients, and transportation of patients to and from the clinics. Thus, the challenge existed to create a vehicle for acknowledging their value. Changes were needed in both the fee structure and documenting procedures.
CHOICES
After deciding that a revised charge system was needed, the literature was reviewed to obtain guidelines for charges in occupational therapy. In 1970, Mae Hightower-Vandamm suggested three philosophies for development of fees for service. First was the philosophy that encouraged the availability of occupational therapy for all who need it regardless of costs. Second was the proposal that occupational therapy charges should be in accordance with those in physical therapy. The third proposal encouraged the use of comparable rates charged in the community. Although the first is altruistic, it does not contain costs. With the second approach, the treatment modalities in physical therapy and occupational therapy vary extensively and no longer offer a practical means to develop fees. And although surveys of fee schedules of hospital departments within the community are necessary to assure a competitive market, such a technique does not assure that expenses will be met and/or that a profit margin will be achieved.1
Laase describes two types of pro...