![]()
II
CENTRAL VENOUS PRESSURE IN CLINICAL USE
![]()
Assessment of Cardiac Output
Publisher Summary
This chapter discusses the assessment of the cardiac output. The most critical transport requirement in the body is that for oxygen. For many tissues, an adequate oxygenation is important. It is the oxygen supply that is limited by a flow in hypotension, and the consequent enforced reduction in oxidative metabolism may damage some tissues. Many factors affect the need of the tissues for oxygen. The important indicators for assessing the adequacy of the cardiac output are found at the capillary level. A good capillary filling with a warm pink skin indicates an adequate cardiac output; a pale or blue cold skin suggests poor perfusion and implies that the output is inadequate. The function of tissues can also be used in the assessment. If brain perfusion is impaired and poor kidney perfusion is revealed by a low urinary output, it is probable that the cardiac output is inadequate for the patient’s requirements. When the cardiac output is low, the blood pressure is usually low and the pulse rate is high.
Even when the physiology and dynamic pathology of the cardiovascular system are understood the practical details of central venous pressure measurement remain to be mastered.
The measurement is not appropriate in every patient but it should be made whenever the cardiovascular dynamics are abnormal. Clinically this may be obvious as pulmonary oedema or, more commonly, as an inadequate cardiac output. Thus an assessment of the adequacy of the cardiac output will often be the first consideration.
If it is decided that the central venous pressure should be measured, then the practical matters of technique and evaluation of the measurements follow.
The most critical transport requirement in the body is that for oxygen. For many tissues an adequate oxygenation is supremely important. It is the oxygen supply that is limited by flow in hypotension (Crowell, 1970) and the consequent enforced reduction in oxidative metabolism may damage some tissues. Many factors affect the need of the tissues for oxygen. Even at rest the individual requirement may be greatly different; from, for example, an abnormal low in myxoedema, to a very high level in fever or during shivering.
Important indicators for assessing the adequacy of cardiac output are found at capillary level. Good capillary filling with a warm pink skin indicates an adequate cardiac output; a pale or blue cold skin suggests poor perfusion and implies that output is inadequate. The function of tissues can also be used in the assessment. If brain perfusion is impaired as shown by a clouded consciousness and poor kidney perfusion is revealed by a low urinary output, it is probable that the cardiac output is inadequate for the patient’s requirements (Motsay et al., 1970). When the cardiac output is low, the blood pressure is usually low (below 90/40 mmHg) and the pulse rate high (an indication of increased sympathetic activity in a heart with normal conduction).
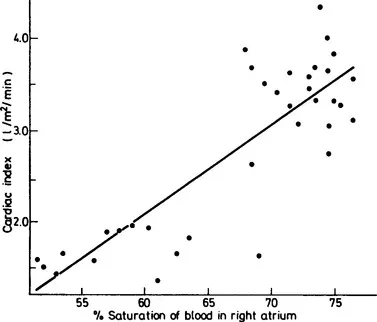
A central venous catheter should be introduced if the patient has an inadequate cardiac output. If the catheter is placed in the right atrium, measurement of central venous oxygen content—an index of tissue oxygenation—can provide a further guide to assessment of the general level of perfusion. Even the less sophisticated measurement of oxygen saturation has a good correlation with the cardiac output (Figure 19) in shock (Lee, et al., 1972). It has also been found suitable as a guide in patients with myocardial infarction (Goldman et al., 1968) and in severely ill cardiac patients (Scheinman, Brown and Rapaport, 1969).
Figure 19 The relationship between oxygen saturation and cardiac output in 36 patients, 13 of whom were considered to be in shock. The output has been standardized as the cardiac index. The correlation coefficient is +0.84 with a regression equation of cardiac index (y) against saturation (x) of y = 0.0974x − 3.76 (Drawn from the data of Lee et al., 1972)
In normal subjects the relationship between the oxygen saturation of blood from the superior vena cava, right atrium, right ventricle and pulmonary artery is very close (Barrat-Boyes and Wood, 1957). This relationship is less close in low cardiac output states; in particular, a blood sample from the superior vena cava tends to have a higher oxygen saturation than do samples from the other sites (Lee et al., 1972; Scheinman, Brown and Rapaport, 1969). However, from any of these sites changes in saturation have the same implication—that a change in perfusion has occurred.
![]()
The Technique of Measurement
Publisher Summary
This chapter discusses the techniques to measure central venous pressure (CVP). A catheter or cannula may be inserted into an external jugular vein to give an approximate value for the CVP. The procedure is simple and convenient. When the central venous catheter is positioned correctly, the pressure reading shows a small fluctuation in time with the patient’s respiration. This fluctuation is because of a slight change in the intrathoracic pressure that occurs with respiratory movements. However, if the catheter is misplaced into the internal jugular vein, respiratory fluctuation may still occur but the reading will be 2–6 cm H2O too high. The reference level is extremely important when measuring central venous or atrial pressures because these differ only slightly from the atmospheric pressure—generally by less than the equivalent of 10 cm of water or saline. The common methods of measurement depend on the presence of a column of liquid between the reference point in the right atrium or central vein and the actual pressure-measuring device.
Insertion of a central venous catheter
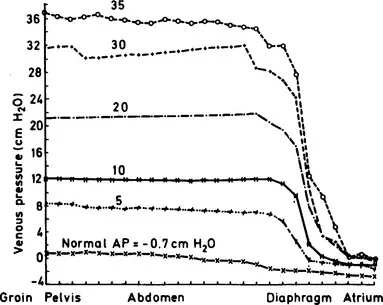
Today most clinicians prefer to avoid the inferior vena cava because of the risk of sepsis in the groin (Bansmer et al., 1958) and because any increase in abdominal pressure makes the readings unreliable (Guyton and Adkins, 1954; Figure 20). The increase in abdominal pressure may be caused by disease—for example, a large amount of ascites; or by a normal situation—such as the enlarged uterus of late pregnancy which may elevate the pressure in the inferior vena cava by as much as 20 cm H2O (Kerr, Scott and Samuel, 1964; Colditz, 1970). Often a catheter is passed from the cubital fossa to the superior vena cava or one of its central tributaries, either by a cut-down, Seldinger technique (Seldinger, 1953; Doty, 1969) or a percutaneous stab (Webre and Arens, 1973). Sometimes more direct approaches to a central vein are made (Figure 21) either by Aubaniac’s (1952) infraclavicular approach to the subclavian vein (Davidson et al., 1963), a supraclavicular subclavian technique (Yoffa, 1965) or a direct approach into the internal jugular vein (English et al., 1969). With any of these techniques the catheter should be radio-opaque or have a radio-opaque line so that the position of the end in the chest may be determined by radiography (Woods et al., 1974).
Figure 20 Diagram of pressure measured at various levels in the inferior vena caval system under conditions of raised intra-abdominal pressure (in dogs). The number above each curve is the pressure in the abdomen in cm H2O. Until the catheter is wi...