
Acute Medicine in the Frail Elderly
Henry Woodford, James George
- 344 pagine
- English
- ePUB (disponibile sull'app)
- Disponibile su iOS e Android
Acute Medicine in the Frail Elderly
Henry Woodford, James George
Informazioni sul libro
Frail older people now contribute the majority of the acute emergency take both medical and surgical. Despite this there is often a lack of confidence and knowledge among doctors and nurses in treating older people in the Emergency Department and on Emergency Assessment Units.From the PrefaceEmergency care of frail older people is challenging but very rewarding. Older patients tend to be complex and therefore their assessment needs to be more extensive and include comprehensive geriatric assessment. It is the extras in their assessment that are not usually needed in younger patients, such as cognitive, functional and social evaluations that make the difference in achieving a better outcome.This book describes the key features of high quality care for frail elderly patients in acute hospital settings. With chapters on assessment and the characteristic non-specific ways that patients tend to present (such as 'confusion', 'collapse query cause' and 'off legs'), this practical guide is ideal to have on-hand. As well as common medical and surgical conditions, it also covers medication management, elder abuse, pressure ulcers and hypothermia, including the physiological changes seen in ageing and ways to define frail patients.Tables, diagrams and images are ideal for quick reference, and key points are summarised throughout the text to aid comprehension, providing doctors, nurses and therapists with both background and essential information to provide the excellent acute care older people deserve.
Domande frequenti
CHAPTER 1
Introduction
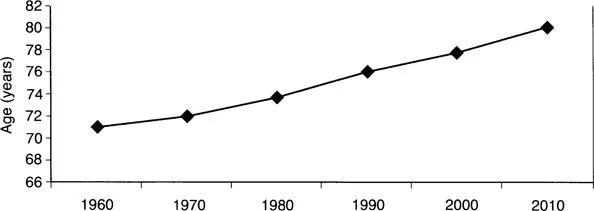
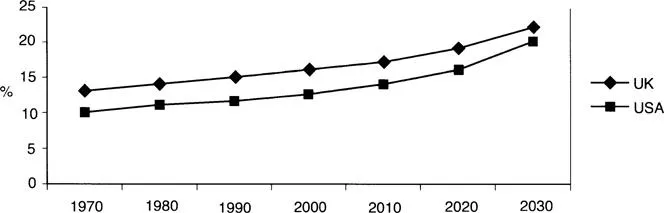
WHAT IS OLD AGE?
CHANGES IN PHYSIOLOGY
Bodily system | Change | |
|---|---|---|
General composition | ↑ | Fat |
↓ | Muscle, bone mass and intracellular water | |
Cardiovascular | ↑ | Systolic blood pressure and risk of arrhythmia |
↓ | Cardiac diastolic relaxation, peak heart rate and maximal cardiac output | |
Respiratory | ↑ | Residual volume |
↓ | Chest wall mobility, respiratory muscle strength and diffusion capacity | |
Renal | ↑ | Risk of dehydration and nephrotoxicity from drugs |
↓ | Glomerular filtration rate and number of glomeruli | |
Neurological | ↑ | White matter lesions, prevalence of hearing and visual impairment |
↓ | Brain volume | |
Gastrointestinal | ↑ | Colonic transit time, gall stones and bowel diverticula |
↓ | Dentition, saliva, sense of taste/smell and liver mass | |
Immunological | ↑ | Autoantibodies |
↓ | Specific antibody production and number of T-cells | |