Frail older people now contribute the majority of the acute emergency take both medical and surgical. Despite this there is often a lack of confidence and knowledge among doctors and nurses in treating older people in the Emergency Department and on Emergency Assessment Units.From the Preface
Emergency care of frail older people is challenging but very rewarding. Older patients tend to be complex and therefore their assessment needs to be more extensive and include comprehensive geriatric assessment. It is the extras in their assessment that are not usually needed in younger patients, such as cognitive, functional and social evaluations that make the difference in achieving a better outcome.
This book describes the key features of high quality care for frail elderly patients in acute hospital settings. With chapters on assessment and the characteristic non-specific ways that patients tend to present (such as 'confusion', 'collapse query cause' and 'off legs'), this practical guide is ideal to have on-hand. As well as common medical and surgical conditions, it also covers medication management, elder abuse, pressure ulcers and hypothermia, including the physiological changes seen in ageing and ways to define frail patients.
Tables, diagrams and images are ideal for quick reference, and key points are summarised throughout the text to aid comprehension, providing doctors, nurses and therapists with both background and essential information to provide the excellent acute care older people deserve.
- 344 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Acute Medicine in the Frail Elderly
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
CHAPTER 1
Introduction
Ageing is the process by which we accumulate cellular damage over time, and this leads to a generalised decline in function, an increased susceptibility to disease and a higher probability of death. It is a complex, multifactorial process and there is much inter-individual variation in the manner and timing of its presentation (seen as differences in ‘biological’ and ‘chronological’ age). It is determined by both internal (i.e. genetics) and external factors (e.g. smoking, diet and sunlight exposure). Ageing is related to reactive oxygen species (or ‘free radical’) production mainly in the mitochondria, which causes damage to cellular structures, such as DNA and proteins (including enzymes).1 We have an imperfect ability to repair our somatic cells’ DNA, resulting in the accumulation of defects. The ‘disposable soma’ theory of ageing explains this as a balance between energy used in repair against that used for reproduction. Wild animals die of predation, starvation and accidents before they have time to age. Therefore, historically, it made more sense to invest resources in producing offspring rather than in maintaining the perfect repair of a doomed body. The ability to live to old age should be celebrated as one of humanity’s achievements, but in the field of healthcare it has created new challenges.
WHAT IS OLD AGE?
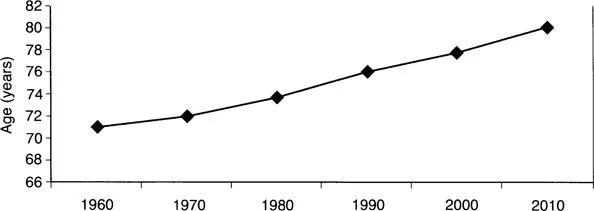
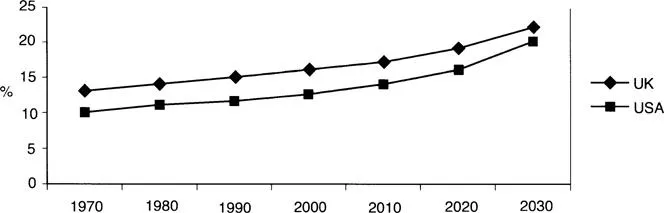
Traditionally, the age of 60 or 65 years has been used to define an older person, which coincided with the typical age of retirement from work. However, over recent years, life expectancy in the developed world has been steadily increasing (see Figure 1.1), and current life expectancy at birth in the UK is around 78 years for men and 82 years for women. The proportion of the population made up of older people is also increasing (see Figure 1.2). Coupled with this has been a reduction in age-related disability levels – that is, our disease-free lifespan has also increased. At the present time, the majority of people aged in their 60s are physiologically very similar to younger adults. The distinction that doctors wish to make is to describe those patients who are physiologically different and require a different approach to that of younger adults. If we were to adopt an age cut-off to achieve this, most of the time it would probably be somewhere over 75 years. The elderly are sometimes classified as the young old’ (60/65–74 years), old old’ (75–84 years) and the oldest old’ (85+ years).
Given the wide variation in the ageing process seen between individuals, age alone is usually insufficient to identify those who need a specialised elderly care’ approach. Other criteria that have been adopted in hospital settings include residing in a care home or presenting with either an acute or chronic geriatric syndrome (confusion, falls, immobility or incontinence).2 Some diagnoses are seen much more frequently in older adults (e.g. dementia) and are usually best cared for by someone experienced in looking after the old. In reality, we use a combination of age, functional status, method of presentation and co-morbidities to define those patients who are best managed under the banner of elderly medicine. The unifying factor is that these patients are considered frail (hence the title for this book). We will discuss frailty later in this chapter. First, let’s outline the physiological changes that accompany ageing.
CHANGES IN PHYSIOLOGY
Ageing is associated with impairments in physiological systems within the body. These are usually compensated for in non-stressful situations, but increased bodily demands imposed by acute illness are more likely to precipitate organ system failure. A summary of the key changes is given in Table 1.1.
Bodily system | Change | |
|---|---|---|
General composition | ↑ | Fat |
↓ | Muscle, bone mass and intracellular water | |
Cardiovascular | ↑ | Systolic blood pressure and risk of arrhythmia |
↓ | Cardiac diastolic relaxation, peak heart rate and maximal cardiac output | |
Respiratory | ↑ | Residual volume |
↓ | Chest wall mobility, respiratory muscle strength and diffusion capacity | |
Renal | ↑ | Risk of dehydration and nephrotoxicity from drugs |
↓ | Glomerular filtration rate and number of glomeruli | |
Neurological | ↑ | White matter lesions, prevalence of hearing and visual impairment |
↓ | Brain volume | |
Gastrointestinal | ↑ | Colonic transit time, gall stones and bowel diverticula |
↓ | Dentition, saliva, sense of taste/smell and liver mass | |
Immunological | ↑ | Autoantibodies |
↓ | Specific antibody production and number of T-cells | |
Bodily composition
As we age, our bodily composition changes, with an increased proportion of fat and less water. Comparing young adults with those in their 80s, body fat increases between 18%–36% for men and 33%–44% for women.3 Fat also tends to be more centrally distributed. This raises the risk of type 2 diabetes and hypertension. Bodily water content falls by around 14% in the elderly compared with young adults, and the reduction mainly affects intracellular fluid.4 There is a gradual reduction in bone mass after the third decade. Older people are at risk of developing osteoporosis. In addition, vitamin D is predominantly formed by the action of sunlight on our skin, and so those who do not go outdoors as often (e.g. the immobile elderly) are at an increased risk of osteomalacia.
Sarcopenia is a term for the reduction in muscle mass, with evidence of reduced muscle strength or reduced physical functioning, that occurs in older age.5 It is likely to be multifactorial in its aetiology, including motor neuron loss, endocrine changes (e.g. sex and growth hormones), nutritional changes, and atrophy secondary to immobility. It is distinct from cachexia (a catabolic state induced by disease). Unfortunately, there is currently no universally accepted method of defining sarcopenia. On average, muscle strength in those aged 60–80 years is 20%–40% lower than that seen in young adults, and it is 50% lower in those aged over 80.6 The observed loss of muscle strength is greater than can be explained by loss of muscle mass alone, suggesting a concomitant reduction in muscle quality.7 However, it is not an irreversible process and high-resistance weight training can lead to significant increases in muscle strength and size even in those aged in their 90s.8
Basal metabolic rate declines because of the reduction in muscle mass. Total energy needs typically fall further because of lower activity levels (e.g. secondary to osteoarthritis). The combined result is a drop in overall energy requirements by approximately 30% from age 30 to age 90. This means less food is necessary to meet energy demands, but protein and micronutrient needs remain similar, which requires a diet relatively high in protein and micronutrients to maintain optimal health. Body weight tends to peak around the age of 60 and gradually decline afterwards. The recommended daily intake for water is around 30 mL/kg/day, and for fibre it is around 30 g/day. Failure to achieve these targets increases the risk of constipation.
Cardiovascular
Ageing is associated with a reduction in elastin content and an increase in collagen and calcium deposition within the arterial walls and myocardium.9 The resulting increased s...
Table of contents
- Cover
- Title Page
- Copyright Page
- Table of Contents
- Foreword
- Preface
- About the authors
- List of abbreviations
- 1 Introduction
- 2 Assessment
- 3 ‘Off legs’: non-specific functional decline
- 4 Confusion
- 5 ‘Collapse query cause’: falls and blackouts
- 6 Surgical care
- 7 Infection
- 8 Cerebrovascular disease
- 9 Chest pain and shortness of breath
- 10 Other presentations
- 11 Medications
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Acute Medicine in the Frail Elderly by Henry Woodford,James George in PDF and/or ePUB format, as well as other popular books in Medicine & Emergency Medicine & Critical Care. We have over 1.5 million books available in our catalogue for you to explore.