
eBook - ePub
Atlas of Cardiac Surgical Techniques E-Book
Frank Sellke, Marc Ruel
This is a test
Condividi libro
- 496 pagine
- English
- ePUB (disponibile sull'app)
- Disponibile su iOS e Android
eBook - ePub
Atlas of Cardiac Surgical Techniques E-Book
Frank Sellke, Marc Ruel
Dettagli del libro
Anteprima del libro
Indice dei contenuti
Citazioni
Informazioni sul libro
Get expert, step-by-step guidance on a wide variety of both open and interventional cardiac surgical techniques. Atlas of Cardiac Surgical Techniques, 2nd Edition, helps you expand your surgical repertoire and hone your skills with a vividly illustrated, easy-to-navigate text and pearls and pitfalls throughout. This revised atlas covers the surgical procedures you need to master, including minimally invasive techniques, robotic surgery, aortic dissection, and much more.
- Seven brand-new chapters cover Hybrid Coronary Revascularization, Aortic Valve Repair Techniques, Transcatheter Aortic Valve Replacement, Robotic Mitral Valve Surgery, Surgery for Hypertrophic Cardiomyopathy, Approaches and Techniques to Extra-Corporeal Membrane Oxygenation, and Pulmonary Endarterectomy.
- Multiple new contributing authors offer a fresh perspective in their areas of expertise.
- A consistent chapter format guides you quickly from surgical anatomy and preoperative considerations through operative steps and postoperative care.
- More than 400 full-color images, line drawings, and intraoperative photographs clearly depict the step-by-step progression of procedures.
Domande frequenti
Come faccio ad annullare l'abbonamento?
È semplicissimo: basta accedere alla sezione Account nelle Impostazioni e cliccare su "Annulla abbonamento". Dopo la cancellazione, l'abbonamento rimarrà attivo per il periodo rimanente già pagato. Per maggiori informazioni, clicca qui
È possibile scaricare libri? Se sì, come?
Al momento è possibile scaricare tramite l'app tutti i nostri libri ePub mobile-friendly. Anche la maggior parte dei nostri PDF è scaricabile e stiamo lavorando per rendere disponibile quanto prima il download di tutti gli altri file. Per maggiori informazioni, clicca qui
Che differenza c'è tra i piani?
Entrambi i piani ti danno accesso illimitato alla libreria e a tutte le funzionalità di Perlego. Le uniche differenze sono il prezzo e il periodo di abbonamento: con il piano annuale risparmierai circa il 30% rispetto a 12 rate con quello mensile.
Cos'è Perlego?
Perlego è un servizio di abbonamento a testi accademici, che ti permette di accedere a un'intera libreria online a un prezzo inferiore rispetto a quello che pagheresti per acquistare un singolo libro al mese. Con oltre 1 milione di testi suddivisi in più di 1.000 categorie, troverai sicuramente ciò che fa per te! Per maggiori informazioni, clicca qui.
Perlego supporta la sintesi vocale?
Cerca l'icona Sintesi vocale nel prossimo libro che leggerai per verificare se è possibile riprodurre l'audio. Questo strumento permette di leggere il testo a voce alta, evidenziandolo man mano che la lettura procede. Puoi aumentare o diminuire la velocità della sintesi vocale, oppure sospendere la riproduzione. Per maggiori informazioni, clicca qui.
Atlas of Cardiac Surgical Techniques E-Book è disponibile online in formato PDF/ePub?
Sì, puoi accedere a Atlas of Cardiac Surgical Techniques E-Book di Frank Sellke, Marc Ruel in formato PDF e/o ePub, così come ad altri libri molto apprezzati nelle sezioni relative a Medizin e Chirurgie & chirurgische Medizin. Scopri oltre 1 milione di libri disponibili nel nostro catalogo.
Informazioni
Section III
Operations for Valvular Heart Disease
Chapter 9
Aortic Valve Replacement
Afshin Ehsan, Frank W. Sellke
Introductory Considerations
Step 1 Surgical Anatomy
- ◆ The aortic valve is the last valve in the heart through which the blood is pumped before it goes to the body. The purpose of the aortic valve is to prevent backflow of blood from the aorta into the left ventricle.
- ◆ The normal aortic valve is tricuspid, with left coronary, right coronary, and noncoronary leaflets. Each leaflet is supported by a fibrous skeleton with a shallow U-shaped configuration. The portion of this skeleton that supports the left coronary leaflet is continuous with the anterior leaflet of the mitral valve, forming the aortic-mitral curtain (annulus fibrosa).
- ◆ Each leaflet is attached just beneath their corresponding sinus of Valsalva. The sinuses of Valsalva are slight dilations of the aorta above the valve that act to create the vortex of blood required for valve closure. The sinuses end at the sinotubular junction, which is the narrowest portion of the ascending aorta.
- ◆ The left main coronary artery arises from the left sinus of Valsalva. Its ostium lies directly posterior, below the level of the sinotubular junction. The left main coronary artery runs to the left, beneath the pulmonary artery. The right coronary ostium is an anterior structure located above the right coronary cusp. Its location tends to be more variable than that of the left main coronary artery.
- ◆ The ventricular septum is located beneath the right coronary cusp and contains the atrioventricular conduction system, which passes below the noncoronary cusp near the right-noncoronary commissure (Fig. 9.1).
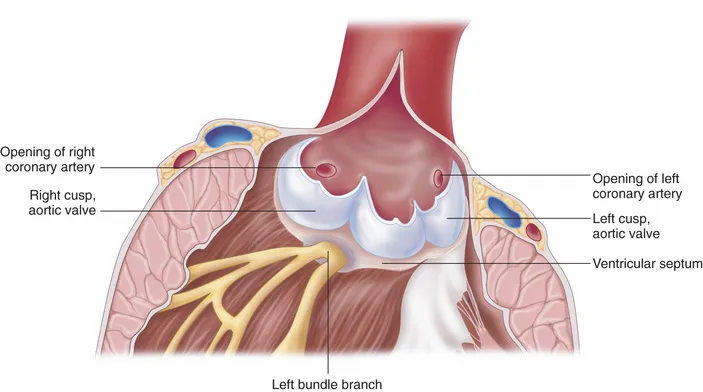 Figure 9.1
Figure 9.1
Step 2 Preoperative Considerations
Indications for Aortic Valve Replacement for Aortic Stenosis
- ◆ In the vast majority of adults, aortic valve replacement (AVR) is the only effective treatment for severe aortic stenosis (AS). Although there is some lack of agreement about the optimal timing of surgery, particularly in asymptomatic patients, it is possible to develop rational guidelines for most patients.
- ◆ In the absence of serious comorbid conditions, AVR is indicated in virtually all symptomatic patients with severe AS. There are many ways in which AVR benefits these patients. These depend partly on the patient's left ventricular (LV) function. The outcome is similar in patients with normal LV function and in those with moderate ventricular dysfunction. The depressed ejection fraction in many of these patients is caused by excessive afterload, and LV function improves after AVR. If LV dysfunction is not caused by afterload mismatch, improvement in LV function and resolution of symptoms may not be complete after valve replacement,1 but survival is still improved in this setting.2
- ◆ Symptomatic patients with angina, dyspnea, or syncope exhibit symptomatic improvement and an increase in survival after AVR.1-6
- ◆ In patients who have severe AS, even those with a low transvalvular pressure gradient, AVR results in hemodynamic improvement and better overall patient functional status.
- ◆ In summary, symptomatic patients with severe AS should undergo AVR. These patients will have improved LV function, reduced or resolved symptoms, and increased survival.
- ◆ Many clinicians are reluctant to proceed with AVR in an asymptomatic patient, whereas others are concerned about conservative treatment of a patient with severe AS. Insertion of a prosthetic aortic valve is associated with low perioperative morbidity and mortality. Despite this, some difference of opinion persists among clinicians regarding the indications for corrective surgery in asymptomatic patients. Irreversible myocardial depression or fibrosis may develop during a prolonged asymptomatic stage, and this may preclude an optimal outcome.5,7 Still others attempt to identify patients who may be at especially high risk of sudden death without surgery, although evidence supporting this approach is limited. Patients in this subgroup include those who have an abnormal response to exercise (e.g., hypotension), those with LV systolic dysfunction, those with marked or excessive LV hypertrophy, and those with evidence of very severe AS.
- ◆ We recommend that asymptomatic patients with an aortic valve area of less than 0.8 cm2 undergo valve replacement. Similarly, any evidence of impaired LV function (e.g., decreased ejection fraction, LV dilation, or significantly elevated LV diastolic pressure at rest or with exercise) is an indication for AVR. In the absence of symptoms, a peak aortic gradient of 70 mm Hg may be an indication for surgery, but this is controversial.
- ◆ Patients with moderate or more AS (mean gradient of 20 mm Hg or higher), with or without symptoms, who are undergoing coronary artery bypass grafting should undergo AVR at the time of the revascularization procedure.
- ◆ Similarly, patients with moderate or more severe AS undergoing surgery on other valves (e.g., mitral valve repair) or the aortic root should also undergo AVR as part of the surgical procedure.
Indications for Aortic Valve Replacement in Aortic Regurgitation
- ◆ AVR is recommended for patients with severe regurgitation in the presence of symptoms or any evidence of pathologic LV remodeling (e.g., impairment of LV function, LV dilation, significant elevation of LV end-diastolic pressure).
- ◆ Symptomatic patients with advanced LV dysfunction (ejection fraction < 0.25 or end-systolic dimension > 60 mm) present difficult management issues. Some patients manifest meaningful recovery of LV function after operation, but many will have developed irreversible myocardial changes. The mortality rate associated with valve replacement approaches 10% in these patients, and the postoperative mortality rate over the subsequent few years is high.
- ◆ AVR should be considered more strongly for patients with New York Heart Association (NYHA) functional class II and III symptoms, especially if symptoms and evidence of LV dysfunction are of recent onset, and intensive short-term therapy with vasodilators, diuretics, or intravenous positive inotropic agents results in substantial improvement in hemodynamics or systolic function. However...