Musculoskeletal Imaging
100 Cases (Common Diseases) US, CT and MRI
Ammar Haouimi
- 244 pagine
- English
- ePUB (disponibile sull'app)
- Disponibile su iOS e Android
Musculoskeletal Imaging
100 Cases (Common Diseases) US, CT and MRI
Ammar Haouimi
Informazioni sul libro
The book includes 100 cases (common and rare) with highly organised radiological description of the diseases.
The cases are grouped into three chapters: Upper Limbs, Neck/Trunk/Spine and Lower Limbs.
High quality images (X-ray, US, CT and MRI).
It covers all imaging modalities including conventional radiology, ultrasound/Doppler, CT scan and MRI.
The topics covered in the book represent the common and important diseases encountered in musculoskeletal imaging.
The material presented for each case provides a thorough and comprehensive description of the disease entity, enabling the radiologist or the clinician to develop a clear concept of the entity through the different imaging modalities that are present.
What is interesting in this book is one case per page. The book can be used as a mean of rapid revision of a large number of cases in a short time or as a test of knowledge by masking the radiological description and diagnosis and trying by using the clinical data and radiological images to describe first the pathology then propose a diagnosis.
Domande frequenti
Informazioni
Case 1
Clinical Presentation
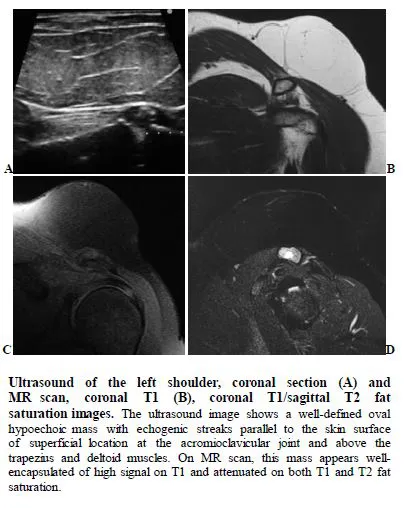
Radiological Findings
Case 2
Clinical Presentation
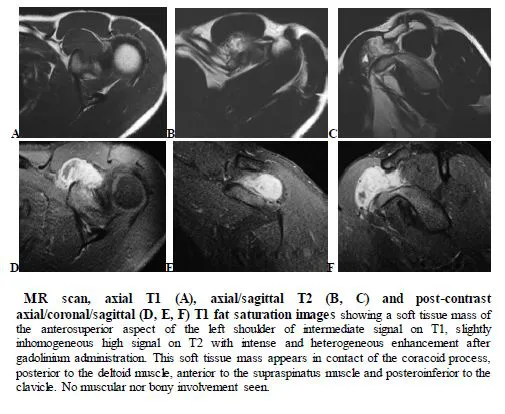
Radiological Findings
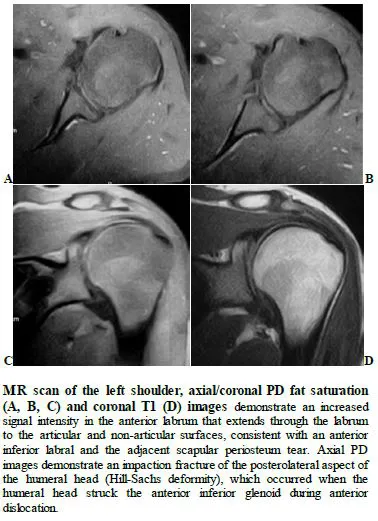
- Perthes lesion of the shoulder: tear of the glenoid labrum with intact scapular periosteum
- Anterior labroligamentous periosteal sleeve avulsion (ALPSA): mobilized labrum remains attached to the glenoid periosteum.
Case 3
Clinical Presentation
Radiological Findings
Case 4
Clinical Presentation
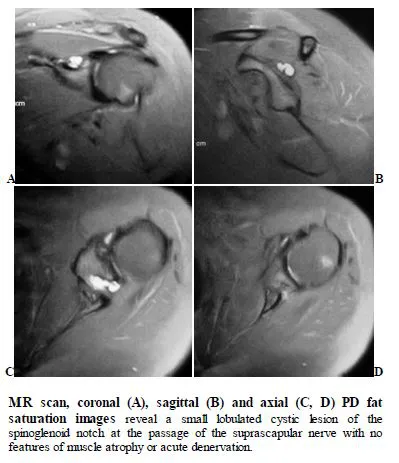
Radiological Findings