![]()
Chapter 1
Examination of the Ear, Nose and Throat
Harold Ludman1 and Patrick J. Bradley2
1King's College Hospital and National Hospital for Neurology and Neurosurgery, London, UK
2Nottingham University Hospitals, Queen's Medical Centre Campus, Nottingham, UK
OVERVIEW
- Taking a history of the symptoms, followed by inspection, palpation and site specific examination of the ENT should be performed in its entirety when a patient first presents with an ENT complaint
- The ability for the non-specialist to perform such an examination is limited because of lack of appropriate equipment and clinical expertise
- Examination of each site; ear, nose, mouth and neck when examined by the non-specialist should be performed in a repetitive systematic manner and the positive findings recorded, thus ensuring that should a patient represent at a later time the previous findings can be reviewed in the light of any new findings
- The specialist examination and investigation is the only definitive current method to ensure a definitive correct diagnosis can be made thus resulting in a correct and appropriate patient management
Examination
Equipment necessary
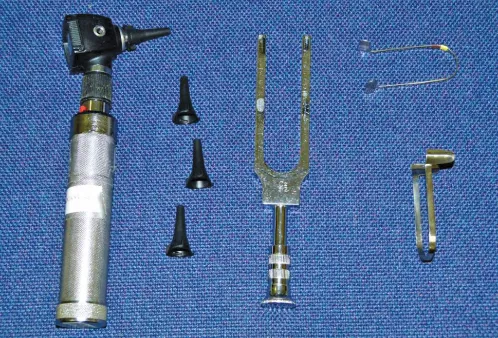
- For the ear—an otoscope (auriscope), comprising a handle, with battery power, light source and cone specula of various sizes and low-level magnification lens; a tuning fork vibrating at 512 kHz (lower frequencies excite vibration sense and higher ones decay too rapidly) (Figure 1.1).
- For the nose—Thudichum's or Killian's nasal speculae.
- For the mouth and oropharynx—Lack's tongue depressors, or spatulae (not as good, because the hand blocks the view and there is a lack of leverage)
- For the neck—a systematic plan is described below.
- For all—Good lighting; ideally from a headlight, or heard mirror and light source (Figure 1.1).
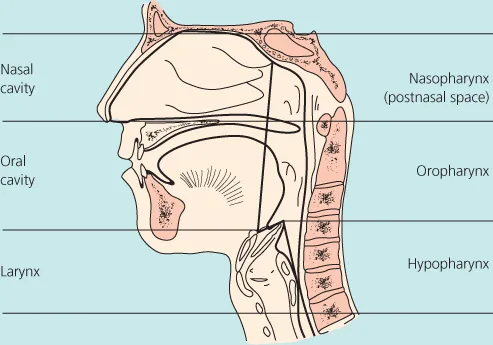
- The larynx, pharynx (nasopharynx [or postnasal space], oropharynx and hypopharynx)—essential parts of the specialty (Figure 1.2) require specialist equipment, which is described in the relevant chapters.
Normal ear anatomy
The external auditory canal
The external auditory canal is 2.5 cm long in adults, extending to the tympanic membrane. The outer one-third passes through elastic cartilage, with hair bearing skin, the inner third is through bone, with no hair and much thinner skin, adherent to the periosteum. The canal is S-shaped and must be straightened by pulling the pinna upward and backward in the adult (straight back in the child) for a better view of the tympanic membrane. The tympanic membrane lies at an angle to the canal, facing forwards and downwards, with an antero-inferior recess, where debris or foreign bodies may collect.
The tympanic membrane (TM or drumhead)
The tympanic membrane consists of a lower pars tensa and an upper pars flaccida, hiding the attic of the middle ear (Figure 1.3). The malleus handle lies in the middle layer of the pars tensa. Its handle runs downwards and backwards from a lateral process—the most easily recognisable structure of the drumhead at its tip (called the umbo), which is in the centre of the pars tensa. From there a cone of light—the light reflex extends antero-inferiorly.
Examination of the ear
Inspection
Compare the pinnae for symmetry.
- Examine the face for evidence of muscle weakness, as in a cranial nerve examination.
- Seek scars, from surgical or other trauma, skin inflammation, swellings, pits or sinuses around the pinna. Scars from previous surgery may be difficult to find.
Palpation
- Feel the mastoid tip, mastoid bone, the pinna itself, and also the parotid and temperomandibular joint area. Pressure on the mastoid tip and the region above and behind it must allow for any pain and tenderness of which the patient complains.
Otoscopy (with auriscope)
Choose a speculum appropriate for the patient's canal. Hold the otoscope with the hand of the same side as the ear to be examined. The otoscope should be held braced against the subject's cheek to avoid injury if the patient suddenly moves. The otoscope should be held with a ‘pencil or pen grip’ (as if writing), with the little finger gently touching the face, to protect against accidental over-insertion. A ‘hammer’ hold of the instrument is wrong (Figure 1.4a and b).
The meatus and then the tympanic membrane should be inspected systematically, with attention to all the pars tensa and the pars flaccida, which may be obscured by a crust. Most importantly, obstruction of view of the pars flaccida.
A sketch of the tympanic membrane showing any observed abnormalities is very useful.
Hearing tests
- Speech material can be used in a quiet room as a Free Field Speech Test (FFST).
- Use conversational material and so-called ‘spondee’ two-syllable words.
- Tuning fork tests in the non-specialist clinic include: the Rinne test and the Weber's test, which usually allow differentiation between conductive and sensorineural hearing loss.
- Pure tone audiometry and tympanometry.
Rinne test—The fork is set vibrating quietly and held adjacent to the external ear canal and then, after a few seconds, the base of the tuning fork is moved and held against the mastoid bone behind ear. The patient has been asked whether he or she can hear the sound in each position and whether it is perceived to be louder at the side of the ear canal or when placed on the mastoid bone behind the ear. A positive Rinne test result indicates that the patient heard the sound louder through the ear canal than through the mastoid bone (air conduction > bone conduction). This positive result is found if the patient has normal hearing in the test ear, or a sensorineural loss. If the patient perceives the ringing to be louder by bone conduction than through the ear canal, drum and ossicles, then there must be a fault in the conducting mechanism. In a conductive hearing loss, the Rinne test is negative (bone conduction > air conduction) (Figure 1.5). Watch out for the so-called ‘false negative’ Rinne test. If the patient has a very severe sensorineural deafness in one ear only, when the vibrating tuning fo...