![]()
1
An International Perspective on Obesity and Obesogenic Environments
W. Philip T. James, Rachel Jackson-Leach and Neville Rigby
1.1 Introduction: the emergence of obesity
The obesity epidemic started becoming a serious public health issue in most western societies only in the early 1980s.1 The problem emerged later in lower income countries as they went through the extraordinary economic and societal changes accompanying what is known as the ‘nutritional transition’. Nevertheless, in countries emerging from extreme circumstances, for example, in post-war Germany or in the richer classes of poor countries, for example, Brazil, women characteristically put on weight first; then the business man’s ‘paunch’ became an index of success. The same persists in African countries where prevailing malnutrition is accentuated by the new fear of ‘slim disease’ - a consequence of HIV infection. Recent studies2,3 show that in affluent societies obesity emerged in children in the early 1980s and since then has become an intense societal concern because no longer could one ignore the fact that environmental pressures must be a major factor in determining this extraordinary development.
Obesity was first highlighted as a major global concern by World Health Organisation (WHO) in 1997, preliminary work having been undertaken by the newly formed International Obesity Task Force (IOTF). In its report the full range of complications from excess weight gain were set out.4 The WHO acceptance of ‘normal’ weights for a population was based on the body mass index (BMI) method for relating weight to height, that is, weight (kg)/[height (m)]2. So people of normal shape and composition but of varying heights had the same BMI, with ‘healthy’ values being taken as between 18.5 and 25, for both men and women of all ages. These values were based on early US insurance figures.1 However, the ready acceptance of the importance of obesity came with the WHO millennium analyses of the major risk factors underlying the burden of premature death and disability from all the major diseases throughout the world.5 The IOTF’s contribution6 showed that the optimum average BMI for a population was only about 21 because the risk of diabetes, high blood pressure and coronary heart disease increased throughout the so called ‘normal’ range. Thus, the risk of diabetes was 5–6 times greater at a BMI of just under 25 than at BMIs of 21. Obese people - that is, with BMIs ≥30 - had more extreme risks.
1.2 The magnitude of the problem
The risks of weight gain include the development of diabetes, heart disease, strokes, high blood pressure, cancers of the breast (post-menopause), colon and rectum, kidney and gallbladder, together with physical handicaps, for example, arthritis. These effects made excess weight, that is, BMIs ≥ 21, rank as the sixth greatest global risk factor for all illnesses accounting for sickness and early death throughout the world! Since then, further analyses in 2006 by WHO, the World Bank and the Centers for Disease Control and Prevention in the United States showed that excess weight is now the third highest risk factor in the affluent world and is within the top 10 risk factors in the regions of the world with the poorest people.7
New IOTF analyses in 2008 showed that there were over 525 million obese adults, with over 1 billion already being overweight (BMIs 25–29.9). This problem is affecting ever younger adults; now in every region of the world, women aged 45-60 years have the maximum rates of overweight and obesity. In the Middle East over 80% of women are affected (of whom >40% are obese), these values exceeding the North American, Latin American, European and Oceania prevalences of >25-35% obesity, with a total prevalence for overweight and obesity of 50-70%. Only Africa and Asia have lower prevalences and even here the middle-aged have obesity rates of 8-15% with totals of 30-40% for BMIs ≥ 25. Men in general have lower values, with North American men showing the greatest prevalence of obesity. In most countries, 50-70% of middle-aged men have BMIs ≥ 25, with obesity rates of >30% in North America, and 15-20% in Latin America, Europe, Middle East and Oceania. Only Asia and Africa have significantly lower rates.
Within more affluent societies there is a strong relationship between the socioeconomic circumstances of a group of children and adults and their susceptibility to gain weight. This also relates to their educational status, with the more affluent and educated groups having much lower obesity rates and a longer life expectancy.
1.3 The basis for the current underestimated burden of obesity
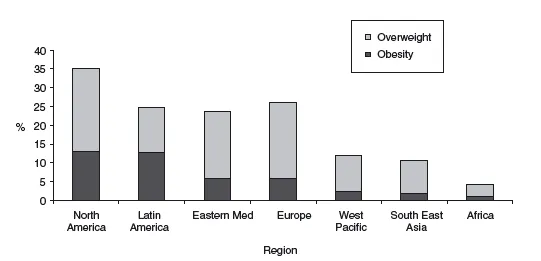
Childhood obesity rates now seem to be accelerating. Four years ago IOTF estimated that 10% of children in the world were overweight or obese8 when the internationally accepted IOTF criteria of overweight were used.9 Yet Figure 1.1 reveals that on average over 15% of the world’s children are now affected; over one-third of North American (including Cuban) children are overweight or obese. Only Africa has an overall prevalence of <10%. The rates are going up remarkably rapidly and now there is clear evidence in affluent societies that even modestly overweight children have a greater lifelong risk of early death and cardiovascular disease, i.e. with high blood pressure, heart disease and strokes.10 Thus, the current burden of ill-health from excess weight gain is an underestimate because the earlier an adult becomes overweight, the greater their future handicap. Current estimates of the burden of overweight and obesity have not included the future impact of such high proportions of overweight children now entering adult life.
The other underestimate of the impact of obesity relates to the fact that Asian communities are far more prone to developing type 2 diabetes and cardiovascular disease than Caucasian adults in western environments.11 This is ascribed to genetic differences, but this is probably incorrect because the body’s susceptibility to adult disease is often programmed by the health and nutritional status of the mother during pregnancy and the child’s growth and well-being in the first 2 years of postnatal life. Thus, European and North American children who are born small and/or grow slowly in the first 2 years of life are much more susceptible to developing selective abdominal obesity with its higher risks of diabetes, cardiovascular disease and some cancers, particularly if they put on excess weight after 2 years of age. This is also evident in India, China and several other developing countries. In India it is being linked to vitamin B12 deficiency and abnormalities of the body’s handling of folic acid metabolism probably exacerbated by low intakes of animal foods.12 Asian adults, at any BMI above 23 (now considered the upper ‘acceptable’ BMI limit for Asians), have a 2–5 fold increased risk of diabetes and high blood pressure. Mexicans are also more susceptible to diabetes and hypertension than US non-Hispanic Whites and acquire the problems rapidly as they gain weight in early adult life.13 So throughout the world the previously termed ‘maturity-onset’ diabetes is now being seen in early adult life and even in children, particularly in the poorer countries.
These data suggest that the majority of the world’s populations may well be more prone to the consequences of excess weight gain than we originally thought. Therefore, given the prevalences of childhood overweight and obesity in the poorer parts of the world (Figure 1.1) we are now confronting a huge global medical problem. Medical costs are rising rapidly; financial analysts show that the medical costs of treatment have increased by 2% per annum above the economic growth of both affluent and poor countries for many decades and about 50% of the increasing medical costs in the United States relate to increasing rates of overweight and obesity. Many lower income countries, previously geared to coping with childhood malnutrition, are already overwhelmed with the problems of the adult chronic diseases. Already over 4 times as many adults die from cardiovascular disease in lower income countries as in Europe, North America, Australasia and Japan. World Bank also shows the irretrievable debts incurred by 40% of Indians’ attempt to cover their medical care costs, and in China the latest parliamentary session recognised the medical plight of the hundreds of millions of poor Chinese rural dwellers as critical. Thus, whether we are dealing with rich or poor countries, the future medical costs are unsustainable. So the challenge is how to convert the political processes which focus on single, short-term solutions to recognise and respond to the need to prevent these problems.
1.4 Individual susceptibility to weight gain and the persistence of obesity
An individual’s susceptibility to put on excess weight is very dependent on his or her genetic make-up. The effect is powerful and explains 50-75% of the difference in the range of weights within any one group living in a particular environment. Thus, in any socio-economic class or educational level those who develop obesity first are the genetically prone to weight gain. Their environmental circumstances or resulting behavioural patterns are still important but it is unwise to blame individuals within a society for their poor health. They can improve their prospects by changing their diet and physical activity patterns, but this is much more difficult for people who are susceptible to weight gain. Also, once adults have gained weight, it is now clear that the brain adapts - perhaps physically in terms of neural pathways - to resist subsequent slimming. This seems to be a strong contributor to the persistence of the epidemic despite the public pressure to lose weight and the billions of dollars spent on weight loss remedies. It is also true that the prevailing environmental pressures are intense; so to overcome these pressures, a family must create its own ‘microenvironment’ to cope. This is a task few can accomplish and there is much inappropriate prejudice relating to both obese children and adults’ excess weight when the most appropriate response is to consider their environmental circumstances and their particular need for help.
1.5 The environmental basis for the obesity epidemic
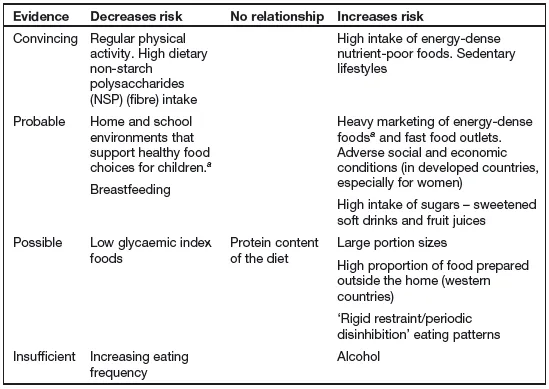
The fundamental environmental basis for the obesity epidemic was recently highlighted by the UK government analysis known as the Foresight report.14 Some implications of this report are summarised in Box 1.1. The emphasis on the normal biological response in terms of weight gain is important because it emphasises the environmental basis for the current epidemic. Therefore, one has to consider both the changes in the energy demand for physical work etc. as well as factors affecting food intake. The latest WHO summary of the factors affecting weight gain is given in Table 1.1. The fall in the demand for physical exertion seems to have come several decades ago in affluent countries with the progressive mechanisation of society, which has reduced the need for physical work. Globally, one of the important factors has been urbanisation with the consequent reduction in the need for the strenuous physical work normally required of peasant farmers. Thus, we calculated that Chinese men and women, formerly living a hard farming life, on transfer to an urban setting but still involved in long hours of building activity or other forms of manual labour, reduced their energy needs by 300–400 kcal/day. This automatically means that this is the reduction in food intake needed by the brain’s automatic regulatory system to prevent weight gain.15 The differences between cycling to work, taking public transport or becoming sufficiently affluent to have one’s own car are also important. Transferring from bicycles - the normal mode of Chinese transport 10 years ago - to public transport saves a further 150 kcal/day or so; having a car reduces the energy demand by about another 100 kcal/day. Thus, the total impact of increasing mechanisation, the constraints of city living and the pressure to sit watching television means that food intakes may need to fall by 400–800 kcal/day for a Chinese adult to compensate for the changes in their working and living conditions: it is a world away from the physical demands of their traditional agricultural subsistence way of life. Indeed, they readily opt for these changes perhaps because the evolutionary demand for intense and/or prolonged physical activity meant that the human race evolved to recognise the value of minimising the demands for physical work.
Box 1.1 Understanding the obesity epidemic and the need for prevention now
1 Obesity is a normal ‘passive’ biological response to our changed physical and food environment.
2 Some children or adults are more susceptible for genetic, social and economic reasons.
3 Overwhelming environmental impact reflects outcome of normal industrial development.
4 Obesity reflects failure of the free market.
5 Obesity is similar to climate change:
- Outcome of numerous societal and industrial developments/forces
- Action now essential - exceptionally difficult to reverse adult obesity
- No single remedy will suffice
- Coordinated central and local government, industrial, societal and individual changes necessary
- Major environmental changes needed - not just individual advice to eat less and walk more
- Immediate action necessary despite many logical remedies remaining unproven
These dramatic changes with urbanisation and technological developments involve both irreversible processes and some options, for example, in the design of the urban physical and social environment. These options can either limit or promote routine and spontaneous physical activity and are primarily determined by central and local governments. These decision makers are, however, influenced by massive industrial pressures attempting to persuade us to use personal motorised transport, personal entertainment and gadgets which minimise the need for any physical activity in the home, in transport or at work. Table 1.2 summarises some of the optional changes in the physical environment which condition everyday physical activity. These changes are heavily influenced by industrial interests and have been very poorly analysed compared with those environmental factors affecting food intake.16
Food intakes should have fallen substantially throughout the world on the basis of the decades’ long progressive fall in the demand for physical work, but for centuries societies everywhere have been concerned with food deprivation. Thus, in several countries intakes have risen and in others they have not fallen enough to match reducing energy needs. The cultural emphasis on food governs adults’ responses to its value and their own perceived need for food as well as their approach to feeding their children. Furthermore, we have evolutionary mechanisms with specific taste buds linked to brain pleasure centres which respond positively to salt, meat, sweetness and fats in the form of essential fatty acids. Now these food components are abundantly available in the industrialised food chain which now forms the most powerful marketing consortium in the world. The global food chain is, therefore, completely inappropriate for a world which is now predominantly sedentary. In a free-market-based world the agricultural, food and marketing sectors continue to maximise their profits, with food outlets and supermarkets filling their shelves with items selected by taste panels. The vast arrays of products are also marketed intensively on the basis of price and they are made available everywhere. ‘Branding’ is also promoted with all the subtlety that psychologists and others can devise. These developments have led to an overwhelming ‘obesogenic’ environment which particularly affects the more vulnerable sectors of society and is transforming the food systems of lower income countries. These pressures operate throughout society with additional lobbying of prime ministers and ministers to ensure that no coherent response is prepared which could threaten the booming food chain profits. These forces are more difficult to combat than the pressures of the tobacco industry.
Table 1.2 Inevitable and optional changes in physical activity.
| Inevitable |
| • Rural to urban transition from agricultural work reducing demand for work |
| • Labour changes from manual to service occupations limiting activity |
| • Mechanisation/computerisation of standard work; also home duties, for example, cooking, washing, cleaning minimising physical exertion |
| Optional |
| • Urban building policies: high intensity or US style sprawl has huge impact on dominance of cars and pedestrian activity |
| • Road and community design affect safe and ready access for play/walking |
| • Office and supermarket location policies determine transport needs |
| • Car/traffic policies based on preference for cyclists/pedestrians? |
| • Policies on free spaces for children’s play; lighting for safety, e.g. for older people |
| • Park/leisure/sports facilities/school physical activity lessons |
| • Reducing the retail food environment index, i.e. the density of fast food outlets in urban environments |
| • Ease of transport of perishable foods into towns/cities |
The British government’s Foresight report set out the immense challenges which require immediate action but far more political resolve is needed than is currently evident. One ray of hope, however, relates to urban planning and the promotion...