Now in a revised and updated new edition which contains seven new chapters, part I of this volume addresses relevant digestive and dental health issues as well as nutritional considerations. Part II covers non-nutritive, high-potency sweeteners and, in addition to established sweeteners, includes information to meet the growing interest in naturally occurring sweeteners. Part III deals with the bulk sweeteners which have now been used in foods for over 20 years and are well established both in food products and in the minds of consumers. In addition to the "traditional" polyol bulk sweeteners, newer products such as isomaltulose are discussed. These are seen to offer many of the advantages of polyols (for example regarding dental heath and low glycaemic response) without the laxative side effects if consumed in large quantity. Part IV provides information on the sweeteners which do not fit into the above groups but which nevertheless may offer interesting sweetening opportunities to the product developer. Finally, Part V examines bulking agents and multifunctional ingredients which can be beneficially used in combination with all types of sweeteners and sugars.
eBook - ePub
Sweeteners and Sugar Alternatives in Food Technology
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Sweeteners and Sugar Alternatives in Food Technology
About this book
This book provides a comprehensive and accessible source of information on all types of sweeteners and functional ingredients, enabling manufacturers to produce low sugar versions of all types of foods that not only taste and perform as well as sugar-based products, but also offer consumer benefits such as calorie reduction, dental health benefits, digestive health benefits and improvements in long term disease risk through strategies such as dietary glycaemic control.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Part One
Nutrition and Health Considerations
1
Glycaemic Responses and Toleration
1.1 INTRODUCTION
Sugars and sweeteners have an important role in the human diet and choosing the right ones in the right amounts can influence health. Knowledge will enable good choices, and further research and understanding of the literature will confirm or deny how good our choices are, and where improvements are possible. Choice is not simply a matter of which is the healthier or healthiest, since the technological properties and economics of sugars and sweeteners impact on which of them can be used suitably in a particular food.
A wide range of potential influence on health is offered by sugars and sweeteners when selected appropriately, as will be evident in detail from other chapters. These include the following:
- A reduced risk of dental caries.1
- Potential for improved restoration of the early carious lesions.2
- A reduction in caloric value that may contribute towards a lower risk of overconsumption, obesity and improved survival.3,4
- Substrate for butyrate production, and potentially reduced risk of colon cancer.5
- The formation of osmolytes efficacious for laxation and lower risk of constipation or accumulation of toxic metabolites.6
- Substrate for saccharolytic and acidogenic organisms in the colon that contribute to prebiosis and ‘digestive health’ potentially including improved immunological function.7,8
Each of these can influence the choice of sugars and sweeteners. Of particular relevance is their impact on glycaemic response and potential to contribute to low glycaemic index (GI) or glycaemic load (GL) diets.
Lowering post-prandial glycaemia and insulinaemia through an appropriate choice of sugars9 and sweeteners,7 together with other low-glycaemic carbohydrates,10 fibre, protein, lower energy intake and exercise,11 can each improve glycaemic control. In turn, this appears to lower the prevalence or risk of developing metabolic diseases including metabolic syndrome, diabetes (and associated complications), heart disease, hypertension, stroke, age-related macular degeneration and certain cancers.12–16
In those who are susceptible, lower glycaemic carbohydrate foods may also benefit appropriate weight gain during pregnancy,17 limit insulin requirements in gestational diabetes,18 potentially allow favourable foetal growth patterns and fat accretion,19 reduce neural tube defects20 and aid recovery from surgery.21
Meta-regression of interventional studies of lower GI or GL diets show a time-dependent lower body weight over a 1-year period22 and supports weight maintenance after weight loss.23 Reduced food intake in humans4 may be partly responsible for weight loss and maintenance. Lowering of body weight improves survival among newly diagnosed diabetes patients,24 and may contribute to longer survival beyond old age as seen in animal studies while lowering glycaemia with isomalt.4
The converse of all aforementioned is that, given the right circumstances, a poor choice of type and amount of all carbohydrates, including sugars and sweeteners, could augment ill health. Attributes of sugars and sweeteners affecting health via the glycaemic response are nutritional and need to be seen in the context of the whole diet. It is appropriate, therefore, to consider the glycaemic aspect of diet and health from ancient to the present and future times – so far as these can be ascertained, explained and envisaged.
1.2 GLYCAEMIC RESPONSE IN ANCIENT TIMES
It is often argued that our genes might not cope with diets that are substantially different from those eaten by our ancestors.25–30 Quite what these diets were or how tolerant ancient genes have become are matters of uncertainty. Successful genes were in existence for both herbivorous and carnivorous diets prior to humankind; however, no early diet appears to have been high glycaemic. Those peoples who would normally consume ‘early’ or rudimentary diets, such as recent hunter–gatherers, experience low levels of diabetes and respond adversely to diets we may now consider high glycaemic.26,31 This is consistent with the notion that early genes were unadapted to high-glycaemic responses, and also consistent with a notion of adaptation having occurred in the people of today's relatively more glucose-tolerant ‘western’ cultures, at least among a large proportion of them. Those not having adapted, contribute to prevalent diabetes and other conditions mentioned that are currently experienced, which is far higher than in either hunter–gatherers or rudimentary horticulturalists or simple agriculturalists or pastoralists.26 For the people of these ‘basic’ cultures and for ‘unadapted’ westerners (easterners or southerners or northerners), a high-glycaemic response remains a health hazard, for which a variety of strategies exist to help them cope.11 Europe has a rich culture and a documented history of its foods, and so we can obtain some idea of how the glycaemic character of diets may have developed over time.
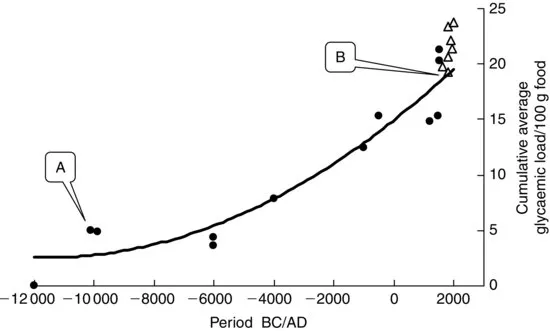
Generally, we may assume diets to partly reflect the foods that can be found or are made available to eat. If this is so, examination of the inventory of foods identified in European history may shed some light on what was eaten and what might now be eaten for optimal health. Such an inventory is provided by Toussaint-Samat32 from which an assessment of the development in the glycaemia character of contemporary diets has been made taking account of the protein, fat, fibre and sources of carbohydrate (Figure 1.1). The picture cannot be accurate but what is clear is a progressive increase in the GL, with a markedly rapid increase in this GL following industrialisation. We cannot be sure of the prevalence of disease in Europe throughout the whole of this timescale, but we would not likely dispute that the prevalence of obesity and metabolic disease is as high now as ever.
Fig. 1.1 Evolutionary adaptation to ancient diets of low glycaemic load may have left mankind genetically predisposed to non-communicable diseases provoked by today's high-glycaemic diets. Based on the history of foods in Europe,32 with calculations by this author (A, agricultural revolution; B, industrial revolution). Open symbols show values post the industrial revolution.
Such a trend is argued to also have occurred throughout more recent times in the United States,25 with recent emphasis on reducing the fat content of the diet, a doubling of flour consumption during the 1980s and an increase overall in sugar, corn syrup and dextrose consumption prior to the end of the millennium.33–35 These together with a lower dietary fibre content of foods34 imply exposure to diets eliciting a high-glycaemic response.
1.3 GLYCAEMIC RESPONSE APPROACHING THE MILLENNIUM
Much of our understanding of the interplay between health and the glycaemic response to foods has arisen from investigations into the dietary management of diabetes. Whereas very low-glycaemic carbohydrate foods such as Chana dahl were used in ancient India for a condition now recognised as diabetes,36 nineteenth century recommendations in western cultures were for starvation diets, which were, of course, non-glycaemic. The drawback of such is obvious and in 1921, high-fat (70%) low-carbohydrate (20%) diets were recommended,37 which by definition would be low glycaemic. A gradual reintroduction of carbohydrate into recommendations for diets for diabetic patients arose as carbohydrate metabolism came under some control using drugs, but mainly because ‘dietary fat’ was recognised to have a causal role in coronary heart disease, to which diabetics and glucose intolerant individuals succumb, more readily in some cases than others.38–41 The metabolic advantages of replacing dietary fat (saturated fat) with high-fibre high-carbohydrate was lower fasting glycaemia, lower total-, HDL- and LDL-cholesterol and lower triglycerides.42–46 Such benefits may in part be related to dietary fibre or its influence on the glycaemic response.47,48 Certainly, the non-digestible carbohydrate in these diets would ensure some degree of lower glycaemia for a given carbohydrate intake and support beneficial effects from lower saturated fat intake.
During these times, the adverse influence of higher glycaemia or more dietary carbohydrate was either unrecognised or the risk was accepted by the medical profession in fear of (or compromise for) the adverse effects of ‘dietary fat’. The adverse influence of higher glycaemia may also have been overlooked due to the apparent benefits of the non-digestible carbohydrate in the high-carbohydrate foods. Indeed, the Institute of Medicine has recommended high-fibre diets to combat coronary heart disease,49 and this builds upon the dietary fibre hypothesis that proposed higher prevalence of diabetes, heart disease and other conditions associate with diets deficient of fibre.50,51 An absence of fibre in high-sugar pro...
Table of contents
- Cover
- Title Page
- Copyright
- Preface
- Contributors
- Part One: Nutrition and Health Considerations
- Part Two: High-Potency Sweeteners
- Part Three: Reduced-Calorie Bulk Sweeteners
- Part Four: Other Sweeteners
- Part Five: Bulking Agents – Multi-Functional Ingredients
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Sweeteners and Sugar Alternatives in Food Technology by Kay O'Donnell, Malcolm Kearsley, Kay O'Donnell,Malcolm Kearsley in PDF and/or ePUB format, as well as other popular books in Technology & Engineering & Food Science. We have over 1.5 million books available in our catalogue for you to explore.