The evidence base for drug treatments in psychiatry ranges from meta-analyses and randomised controlled clinical trials to single case reports, and from NICE guidelines to individual SPCs. Where do you look for information when transferring a patient from one drug to another? Where do you find a clear overview when dealing with a complex patient (e.g, with co-morbid epilepsy or liver disease or HIV infection)? Where can you seek advice on prescribing psychotropics during pregnancy? The Maudsley Prescribing Guidelines in Psychiatry! The leading clinical reference for handling prescribing problems as encountered in daily practice and for formulating prescribing policy.
Evidence-based and written by experts
This book is the essential guide for anyone responsible for prescribing, dispensing or administering drugs for patients with mental health disorders. All the evidence has been reviewed and summarized succinctly by an expert team of psychiatrists and pharmacists.
New content and improved format
This new edition makes greater use of tables and boxes to facilitate quick reference and includes new sections on cytochrome-mediated interactions and psychiatric side effects of non-psychotropic drugs.
Clinically relevant
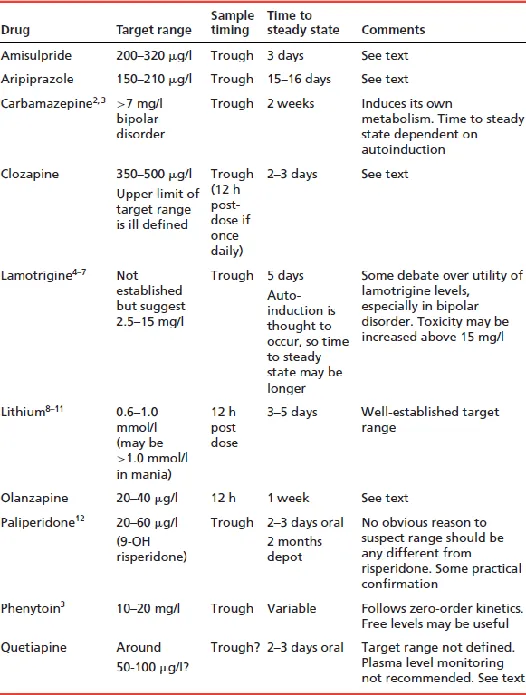
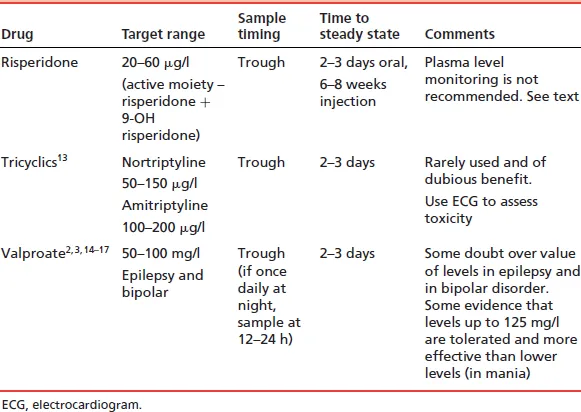
Chapters address plasma monitoring, schizophrenia, bipolar disorder, depression and anxiety, children and adolescents, substance abuse and special patient groups. Each section has a full reference list. The book covers prescribing drugs outside their licensed indications and their interaction with substances such as alcohol, nicotine and caffeine.
Useful for all levels of experience
Trainees will gain important information regarding the rational, safe and effective use of medications for patients with mental illness. Experienced clinicians will find excellent guidance regarding more complex issues that they may not encounter regularly.
Why the Maudsley Prescribing Guidelines in Psychiatry?
Long recognized as an international trailblazer in mental health care, the Maudsley Hospital earned its reputation for excellence in both in-patient and community care. It is highly regarded for its research, and pioneered the use of clinical neuroscience. You can trust The Maudsley Prescribing Guidelines in Psychiatry to be scientifically sound and clinically effective.