eBook - ePub
Male Infertility in Reproductive Medicine
Diagnosis and Management
- 205 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Male Infertility in Reproductive Medicine
Diagnosis and Management
About this book
This useful illustrated text summarizes for an audience of clinicians in Reproductive Medicine the practical essentials of what they need to know about diagnosis and management of the infertile male patient, whether they need to instruct or liaise with a colleague or undertake the procedures themselves.
Information
1
The Pathophysiology of Male Infertility
Pallav Sengupta and Chak-Lam Cho
KEY POINTS
• Pathophysiology of male infertility involves complex multivariate mechanisms.
• Dysregulations of hormonal axes and endocrine cross-talks adversely affect male reproductive functions.
• Testicular disruptions directly impair semen parameters.
• Posttesticular impairments afflict spermatozoal maturation and transport.
Introduction
The male reproductive system apparently possesses simplistic functions so as to produce sperm and testosterone, but the underlying mechanisms are far more complex and yet to be completely revealed. Such elusive mechanisms of male reproductive functions have led to poor understanding of the actual causatives of male infertility in about 50% of the cases [1]. Disruption of male fertility may be reflected by impaired sperm parameters through multivariate factors at different levels [2,3,4]. Etiologies of male infertility may act at the pretesticular or neuroendocrine regulatory levels. Other factors may directly affect intratesticular sites, thereby afflicting the functions of Sertoli cells, Leydig cells, and germ cells. Disruptions can also occur at the posttesticular strata, impairing sperm maturation and transport. Besides the conventional concept of pathophysiology of male infertility, there is advent in male reproductive immunology as well as reproductive genetics and epigenetics, modulations of which may induce varying forms of impairment to the male fecundity. Proper evaluation of male infertility at different levels is essential for its effective management. Targeted treatment to specific male factor with or without assisted reproductive techniques (ART) may be adopted for management of male infertility [5].
This chapter is a concise synopsis of the pathophysiology of male infertility merging the classical and modern postulations. It summarizes the concepts of male reproductive functions and their regulatory factors. Finally the mechanisms by which impairment of the reproductive functions or their regulators, individually or in concerts, leading to male infertility are illustrated.
Male Reproductive Physiology: An Overview
Pristine perception of both morphology and physiology of male reproductive system facilitates conceptualization of the complex pathophysiological mechanisms of male infertility. The male reproductive system has three fundamental functions: Production of spermatozoa (spermatogenesis) and hormones (steroidogenesis), as well as storage followed by ejaculation of the sperm into the female reproductive tract [6]. However, accomplishment of these functions require orchestrated action of the testicular cells including the germ cells, Sertoli cells, and Leydig cells in response to the endocrine regulation. The male reproductive system along with its regulatory entity comprises of brain centers, which regulate pituitary release of gonadotropins and sexual behavior; a pair of testes, which produce sperm and hormones; a ductal system (vas deferens and epididymis), which stores and transports sperm; accessory sex glands (seminal vesicles, prostate, and bulbourethral glands) to support sperm viability; and the penis [7].
Spermatogenesis and steroidogenesis are under endocrine regulation via the pituitary gonadotropins, luteinizing hormone (LH) and follicle-stimulating hormone (FSH) [8]. The hypothalamus is known to be the center of information processing as per external and internal cues. Via the pulsatile release of gonadotropin-releasing hormone (GnRH), it stimulates the secretion by anterior pituitary, LH and FSH, which binds to receptors on the Leydig cells, and Sertoli cells, respectively. Leydig cells reside within the interstitial compartments and produce testosterone. Sertoli cells lie along the lining of the seminiferous tubules, supporting the germ cells to develop through the stages of spermatogenesis. Sertoli cells have receptors for both FSH and testosterone and produce estradiol at low levels. Another contribution of the Sertoli cells is the productions of glycoprotein hormones (inhibin, activin, and follistatin) that modulate FSH secretion [9]. Testosterone is the main androgen that sends feedback to the hypothalamus and pituitary, regulates spermatogenesis directly, monitors sexual behavior, and serves as the primary male sex hormone that aids primary and secondary sex development.
The duct system, comprising of epididymis, vas deferens, and urethra, stores the sperm until they acquire the capability to fertilize with sufficient motility and then transports them to the female genital tract through the penis [6].
Alterations in one or more of the components of the reproductive system are accompanied by modulations in other reproductive organs and their endocrine regulations.
Etiologies of Male Infertility
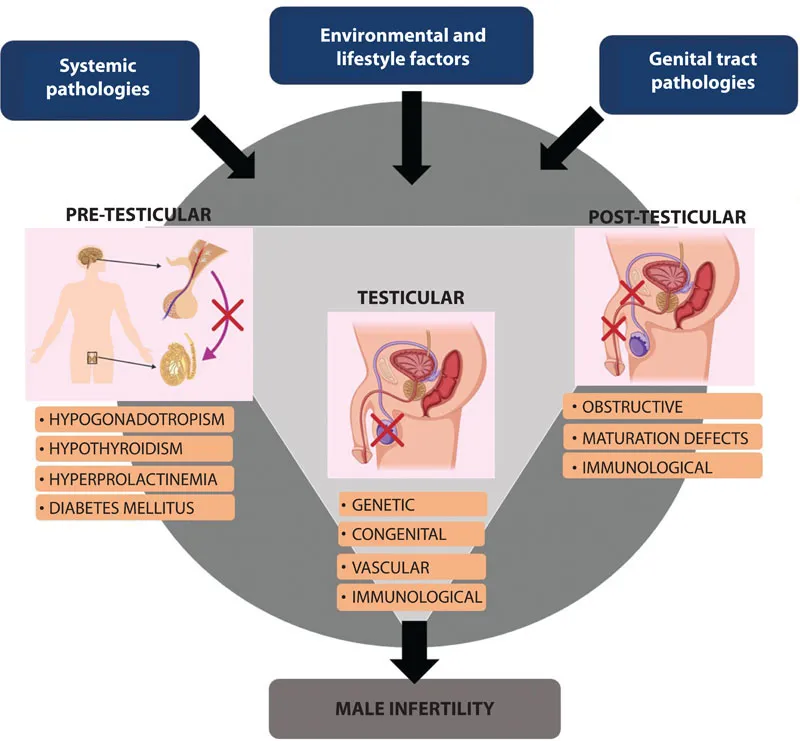
The clinical definition of “infertility” itself not only often poses a conceptual enigma that both subfertile and infertile couples are put under the same category but also refers to failure in attaining pregnancy within the first year of unprotected intercourse. However, many subfertile couples actually may not conceive within this stipulated time and are included under the definition of being infertile [10]. In addition, among all the cases of male infertility, about 60%–75% are idiopathic and remain undiagnosed [11]. Diagnosis of male infertility probably covers a number of different etiologies, which again is a mechanistic paradox and several hypotheses attempt to explain the multivariate causes of the same. The physiological disruptions resulting in male infertility may be related to failure in sperm production, impaired sperm morphology and functions, problems in transmission along the duct system through the penis during ejaculation, secretory disturbances of the accessory glands, and endocrine imbalances. There lies an array of concepts to justify these events individually or in combinations and most of the time, the exact mechanism is difficult to specify. In many cases, male infertility remains just a mystery. The contributing factors ranges from severe to moderate pathological conditions, systemic causes, environmental factors, lifestyle factors, and metabolic distress to oxidative stress (Figure 1.1). This chapter aims to address the perplexity unveiling the physiological mechanisms paving the way to male infertility, explaining every strata of male reproductive functions at the pretesticular, testicular, and posttesticular levels.
Pretesticular Pathophysiology
Immaculate coordination of the hypothalamic-pituitary-testicular axis with other related hormones determine functioning of the male reproductive system. The hypothalamus via its pulsatile secretion of GnRH stimulates the pituitary gonadotropins, LH, and FSH, which regulate testicular steroidogenesis and spermatogenesis. Inhibin and activin from the testes in turn operate feedback mechanisms that influence the secretion of both hypothalamic GnRH and subsequent pituitary gonadotropins [12].
Research since the last decade, procures that besides the pivotal classical scheme of the hypothalamic-pituitary-gonadal (HPG) axis, there are several other components playing vital roles in the regulation of male reproductive functions. Among these are the groups of small RFamide peptides consisting of the motif Arg-Phe-NH2 at C-terminus, namely, gonadotropin-inhibiting hormone (GnIH) and its related peptides [8]. Another essential 54-amino-acid peptide, Kisspeptin, encoded by the KiSS-1 gene, has been identified. This peptide, which activates the G protein–coupled receptor (GPR54) in the hypothalamus, is reportedly a major trigger for puberty and can supposedly even kindle precocious puberty in men [13].
HPG axis may be disoriented by the influence of an inestimable number of internal and external cues, the most common being via the stress hormones, several adipokines, and the opioid system. A disrupted HPG axis results in inadequate sex steroids and inhibin production and in turn, loss of negative feedback to regulate hypothalamus and pituitary secretions. Consequently, there is an increase in serum activin and unregulated release of GnRH and gonadotropins [14]. This undesired elevation of LH and FSH culminates in male reproductive dysfunctions [15]. Hence, dysregulation of the HPG axis actually modulates concentrations of gonadal hormones and alters the sensitivity of their respective hippocampal receptors, resulting in disoriented hormone-receptor signaling and abnormal elevation in neuronal GnRH, LH, and activin signaling [16]. Stress may also induce elevated levels of reactive oxygen species (ROS), which may trigger oxidative stress (OS). This may lead to lipid peroxidation (LPO) in Leydig cells and germ cells, disrupt lipoproteins, fragment proteins, and inhibit steroidogenic enzyme activities [17]. OS mediates its detrimental effects on male fertility by reduction in testosterone production by affecting Leydig cells or indirectly via disruptions in endocrine regulations of hypothalamus or anterior pituitary [18].
Interruption or ceased GnRH release and subsequent inhibition of LH and FSH secretions lead to hypogonadotropic hypogonadism (HH). Secondary and tertiary HH owing to hypothalamic and pituitary hormones deficiencies, respectively, are different from primary or testicular dependent factors. Secondary or tertiary HH is characterized by normal or low gonadotropin levels with low testosterone concentration [12]. Congenital abnormalities resulting from GnRH deficiency can either occur singly (normosmic congenital HH) or along with hyposmia or anosmia, which is called Kallmann syndrome. Besides testosterone insufficiency, fertility problems, and anosmia, patients with Kallmann syndrome often experience other neurologic and cardiac disorders. Hypogonadism is thus a threat to male fecundity and systemic functions and can be caused by various factors including aging [19], obesity [20], and type 2 diabetes mellitus [21]. Steroidogenesis gradually declines with aging and reports suggest men older than 60 years general...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Table of Contents
- Preface
- Acknowledgments
- Editors
- Contributors
- 1. The Pathophysiology of Male Infertility
- 2. Assessment and Diagnosis of the Male Infertility Patient
- 3. Semen Analysis
- 4. Ultrasound Imaging of the Infertile Male
- 5. Genetic Causes of Male Infertility
- 6. BMI and Male Fertility
- 7. Role of Sperm DNA Damage in Male Infertility Assessment
- 8. Sexually Transmitted Infection and Male Infertility
- 9. Klinefelter Syndrome
- 10. Varicocele
- 11. Azoospermia
- 12. Erectile Dysfunction
- 13. Oxidative Stress: Relevance, Evaluation, and Management
- 14. Medical Treatment of Male Infertility
- 15. Lifestyle Management Approaches to Male Infertility
- 16. Surgical Management Techniques for Male Infertility
- 17. Sperm Banking
- 18. Intrauterine Insemination with Homologous Sperm
- 19. Intracytoplasmic Sperm Injection
- Index
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Male Infertility in Reproductive Medicine by Botros Rizk, Ashok Agarwal, Edmund Sabanegh Jr., Botros Rizk,Ashok Agarwal,Edmund Sabanegh Jr.,Edmund S. Sabanegh Jr., Botros Rizk, Ashok Agarwal, Edmund S. Sabanegh Jr. in PDF and/or ePUB format, as well as other popular books in Medicine & Gynecology, Obstetrics & Midwifery. We have over 1.5 million books available in our catalogue for you to explore.