- 178 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
When a patient presents to the emergency department, in the GP practice, or in the outpatient clinic with a range of clinical signs, the chest x-ray is one of the most valuable diagnostic tools available to the attending physician. Accurate interpretation and understanding of the chest x-ray is therefore a crucial skill that all medical students an
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
CHAPTER 1
The systematic approach
There are two basic elements to the systematic interpretation of a chest radiograph. The first is the structure of the system itself and this chapter describes the sequence of interpretation I have developed over the years. Whether you adopt this system or develop your own, it is essential to be disciplined and not deviate from a structured approach. Train yourself to examine anatomical structures in strict order because deviation will risk missing important information. A classic example is your eye being drawn to an obvious abnormality. You note the abnormality and it is easy to consider ‘job done’ ignoring further critical examination. This happened recently when a radiographic diagnosis was considered complete after multiple rounded shadows were detected in the lung fields. These were well defined, variable in size and clearly represented metastatic malignant disease. Unfortunately, the right mastectomy, readily visible on the radiograph and the likely source of the metastatic deposits, was missed and this was simply because the breast shadows were not examined specifically as part of a systematic approach. I have known osteolytic lesions in ribs (accompanying an obvious lung mass) to be missed for exactly the same reason. So, develop a sequential system of observation and do not deviate from it.
The second element is to ‘problem-solve’ as you follow your systematic interpretation. By this I mean ask specific questions at each stage of the examination. Is an anatomical structure of normal size, is it correctly positioned and are its borders well defined? What are the detailed features of any pulmonary infiltrate – distribution, size and shape of component shadows, presence of calcification and so on? In other words, go in search of information and do not just wait for it to hit you in the eye – this is a basic, generic skill of clinical medicine.
There is a third element that will accrue with experience and this is ‘pattern recognition’ – an ability to recognize heart failure because you have seen the pattern hundreds of times and recognize it. Pattern recognition is another generic skill of the art of clinical medicine and should not be disparaged but use it warily and do not allow yourself to abbreviate the systematic approach – even the most experienced of us has been caught out by ignoring this fundamental maxim.
Here is the system I follow.
BASIC OBSERVATIONS FIRST
• Note the patient’s name, age and ethnic background. These details may provide clues to the possible diagnosis.
• What is the date of the radiograph? A stunning radiographic diagnosis is far more relevant to patient care if the X-ray is current rather than 2 years old.
• Has the radiograph been taken in postero-anterior (PA) or antero-posterior (AP) projection? If the latter, then it is impossible to comment accurately on heart size.
• How centred is the image? Look at the sterno-clavicular joints when making this assessment. The right and left sterno-clavicular joints are equidistant from the mid-line in the normal chest X-ray shown in Fig. 1.1 (arrowed) and this is a well-centred radiograph. A rotated film will distort the appearance of all anatomical structures, particularly those within the mediastinum, and interpretation may be impossible if the image is significantly skewed.
• Next, decide on the degree of radiological penetration of the image. Ideal penetration applies when you can see vertebral bodies clearly through the heart shadow. Sometimes a softer film helps in defining pulmonary infiltration and, in these days of digital images, it is possible to manipulate the window level in order to optimize penetration. Figure 1.1 is an example of near-perfect X-ray penetration.
• Finally, examine the alignment of the ribs. In Fig. 1.2 the ribs are horizontal with the anterior and posterior parts of each rib shadow virtually overlying one another. This is an AP X-ray that has been taken with the patient lying back rather than sitting (lordotic). The mediastinum and the hemidiaphragms are very distorted and interpretation is unreliable, a situation exacerbated by the fact that the film is significantly underpenetrated.
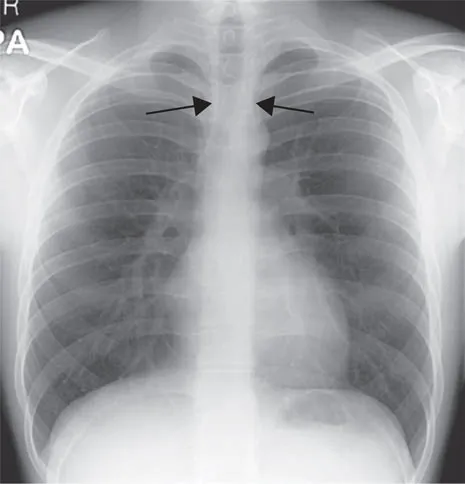
Figure 1.1 Normal chest X-ray.

Figure 1.2 An underpenetrated lordotic chest X-ray. The horizontal appearance of the ribs is the clue to imperfect patient positioning.
Accurate radiographic interpretation is reliant upon the quality of the X-ray. It is vital to assess penetration, centring and position of the patient before drawing conclusions from the radiographic appearances.
Figure 1.3 illustrates the characteristic acute angle between posterior and lateral ribs in a patient with pectus excavatum. Note the ‘fuzziness’ adjacent to the right heart border, which is a normal accompaniment of this anatomical variant. Recognition of pectus exc...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Table of Contents
- Preface
- Acknowledgements
- List of abbreviations
- 1 The systematic approach
- 2 The mediastinum and the hila
- 3 Consolidation, collapse and cavitation
- 4 Pulmonary infiltrates, nodular lesions, ring shadows and calcification
- 5 Pleural disease
- 6 The hypoxaemic patient with a normal chest radiograph
- 7 Practice examples and ‘fascinomas’
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Making Sense of the Chest X-ray by Paul Jenkins in PDF and/or ePUB format, as well as other popular books in Medicine & Internal Medicine & Diagnosis. We have over 1.5 million books available in our catalogue for you to explore.