Objectives
To review the basic histological knowledge of the nervous system from a functional (neurological) perspective
To organize the nerves, nuclei and tracts of the nervous system into functional systems
In the Introduction, Crash, pilot and astronaut, executes a number of intricate tasks in response to input from several sensory systems: tactile, muscle and joint, visual, vestibular and auditory. He reacts to all of these stimuli appropriately and performs highly accurate and skilled motor movements. Pathways were sketched for the sensory input and for executing the motor movements.
How does the brain process all this information? Which parts of the nervous system are involved in the exquisite motor control required to fly a jet aircraft or pilot a space craft? Where in the ‘brain’ are the integration and decision-making functions carried out?
A neurologist’s view of the nervous system is one of functionality – are all the components operational in order to receive information, analyze and assess its significance and produce the appropriate action? If not, the task of the physician is to determine where the problem is occurring and what is its most likely cause – the localization of the lesion and its possible etiology.
In order to determine where, the localization, one needs to have knowledge of the anatomy and physiology of the nervous system. This chapter will provide that information from a functional perspective, but the student should expect to consult other resources – details of neuroanatomy, neurophysiology and neuropathology – to supplement this presentation (see Suggested Readings and the Annotated Bibliography). One needs this knowledge to understand the significance of the findings of the neurological examination, which is outlined in the next chapter.
Determining the likely cause, the etiology, requires knowledge of disease processes. This determination is based initially on the nature of the symptoms and the history of the illness – how long the problem has been occurring (acute, subacute, chronic) and how the symptoms have evolved over time. The task of the practitioner – physician, resident or student – will be to determine what disease process (e.g. infectious, vascular, neoplastic) is occurring and its pathophysiology, and to identify diseases that most likely account for the patient’s signs and symptoms.
Laboratory investigations, including blood work, special tests (e.g. disease-specific antibody levels) and particularly neuroimaging, usually provide additional information to help pinpoint the localization of the disease and often limit the possible list of most likely diseases.
Lastly, the neurologist will synthesize the patient’s history and the symptoms with the signs found on neurological examination as well as the additional information provided by the investigations to come up with the definitive diagnosis. This diagnosis allows for a therapeutic plan and some idea of the likely outcome: the prognosis. All of this must be communicated sensitively to the patient and family in a way that can be readily understood. (A sample case exemplifying this approach is presented in Chapter 3.)
1.1Neurobasics
The nervous system is designed to receive information, analyse the significance of this input and respond appropriately (the output), usually by performing a movement or by communicating ideas through spoken language. In its simplest form, this process would require a minimum of three neurons, but as we come up through the animal kingdom, the complexity of analysis increases incredibly. This evolutionary development culminates in the human central nervous system (CNS), with all its multifaceted functions.
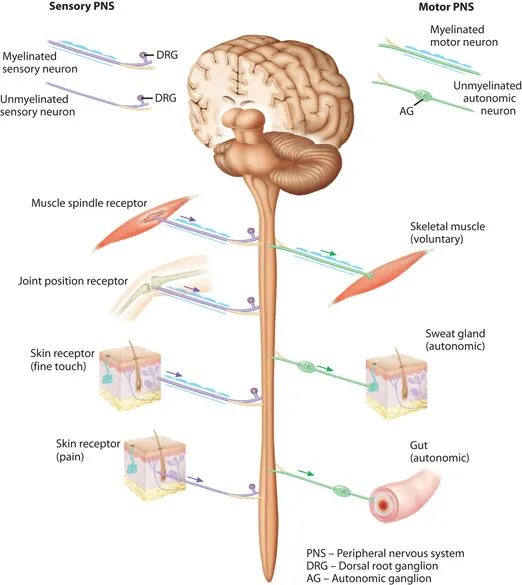
The nervous system consists of two divisions (Figure 1.1), a peripheral component, called the peripheral nervous system, the PNS, and a central set of structures, called the central nervous system, the CNS. The PNS consists of sensory neurons and their fibers, which convey messages that originate from the skin, muscles and joints and from special sensory organs such as the cochlea (hearing); it also carries the motor nerve fibers that activate the muscles. The autonomic nervous system, the ANS, is also considered part of the PNS; it is involved with the regulation of the cardiac pacemaker system and of smooth muscle and glands, including some control of bowel and bladder functions. The CNS consists of the spinal cord, the brainstem and the brain hemispheres. The CNS adds analytic functionality and varying levels of motor control, culminating in a remarkably intricate capacity for ‘thinking’ forward and backward in time, consciousness, language and executive functions, processes performed in different areas of the cerebral cortex.
Figure 1.1Overview of the nervous system – CNS, PNS and ANS. Sensory fibers, coloured purple, convey information towards the CNS (afferent) from receptors in skin and muscle. Motor fibers, coloured green, carry instructions away from the CNS (efferent) to muscle and via autonomic ganglia to glands and viscera.
1.1.1The Neuron
A neuron is the basic cellular element of the nervous system. In the most simplistic language of today’s electronic world, each of the billions of neurons in the human CNS is equivalent to a unique microchip, possessing a specific information processing capacity. Like other cells, the neuron has a cell body (the soma or perikaryon) with a nucleus and the cellular machinery to be its nutritive centre. Morphologically, it is the cellular processes – dendrites and axon – that distinguish a neuron from other cells. The electrochemical nature of its membrane, whereby the interior of the cell and its processes have a negative charge, is a characteristic feature of the neuron (see Figures 11.1, 11.2 and 11.3). The synapse, the electrochemical communication between neurons, is the other unique feature of nervous tissue (discussed in Section 1.1.4).
The typical neuron in the CNS (Figure 1.2a) has dendrites that extend from the cell body for several microns. Dendrites receive information from other neurons at specialized receptor areas, the synapses, some of which form small excrescences on the dendrites, called synaptic spines (discussed in Section 1.1.4). More complex neurons have an extensive arborization of dendrites and receive information from perhaps hundreds of other neurons. Neurons of a certain functional type tend to have a typical configuration of their dendrites and group together to form a nucleus (somewhat confusing terminology!) in the CNS, or a layer of cortex (e.g. the cerebral or cerebellar cortex). Brain tissue is traditionally fixed in formalin for the purpose of study, and neuronal areas (e.g. the cortex) become grayish in ...