eBook - ePub
Spasticity Management
A Practical Multidisciplinary Guide, Second Edition
- 304 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Spasticity Management
A Practical Multidisciplinary Guide, Second Edition
About this book
Spasticity is a common symptom that arises in a wide range of neurological conditions. Unfortunately, a poor understanding and inadequate management of spasticity often results in it having a greater impact on patients than necessary. Using a multidisciplinary approach, Spasticity Management: A Practical Multidisciplinary Guide provides the essenti
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
PART 1
Chapters
1 What is spasticity?
Jonathan F Marsden
2 Assessment of the individual with spasticity
Valerie L Stevenson, Katrina Buchanan, Elizabeth Keenan and Louise Jarrett
3 Provision of education and promoting self-management
Louise Jarrett and Elizabeth Keenan
4 Physical and postural management of spasticity
Katrina Buchanan and Susan Hourihan
5 Oral medication
Valerie L Stevenson
6 Focal treatments, including botulinum toxin
Rachel Farrell and Katrina Buchanan
7 Intrathecal baclofen and phenol
Valerie L Stevenson, Elizabeth Keenan and Louise Jarrett
8 Transitioning young people with spasticity from paediatric to adult services
Sarah Perides and Margaret Kaminska
9 End-of-life care and managing spasticity
Jane Neerkin and David Oliver
1
What Is Spasticity?
Hypertonia and Spasticity
Spasticity: Definitions and Associated Symptoms
Stretch Reflexes
Modulation of the monosynaptic stretch reflex
Factors affecting stretch reflex size
Stretch reflex changes during functional movement
Long-latency stretch reflexes
Stretch reflexes and spasticity
Pathophysiology of Spasticity
A lesion to UMN pathways
A reduction in inhibitory spinal cord circuits
Adaptive changes in the properties of the motor neurons and spinal interneurons
Spasticity and Functional Movement
Modulation of Spasticity by Descending and Peripheral Afferents
Changes in Passive Stiffness
Changes in the intramuscular protein titin
Changes in muscle fascicle and sarcomere length
Changes in the amount and structure of connective tissue
Changes in the number of cross-bridge attachments in the muscle at rest
Distinguishing Between Neural and Nonneural Stiffness
Passive stiffness and function
Fibrosis and contractures
Co-contraction
Clonus
Spasms
Associated Reactions
The Positive Support Reaction
Spasticity in Context
Conclusions
References
‘Spasticity’ means different things to different people. The individual with spasticity will no doubt think of it in terms of their own symptoms and how these affect them, whereas physicians and other healthcare providers often consider spasticity as a neurological impairment. When considering how best to manage a person’s symptoms or reduce the impact of these on their daily life, it may seem unimportant to think about the underlying neurophysiological changes secondary to their neurological condition. However, a sound knowledge of underlying physiology is extremely important for all members of the multidisciplinary team. This knowledge will not only guide the team in devising the most appropriate management plan for an individual, but will also allow them to provide clear and relevant education to the person with spasticity and, if appropriate, their families and carers. This provision of education and promotion of self-management is instrumental in the overall success of any spasticity management programme. The muscle stiffness of spasticity, often with associated spasms, is an extremely common symptom seen in many neurological conditions, including head or spinal cord injury, stroke, cerebral palsy and multiple sclerosis. It is also a significant feature in a number of rarer conditions, such as hereditary spastic paraparesis. Due to the diversity of causes, it is a problem faced by many people of all ages and backgrounds. Several of these disorders predominantly affect young adults or are lifelong conditions, in contrast to stroke, which is predominantly a disorder of older age. It is therefore essential that all health workers, whether based in hospitals or in the community, be equipped with a degree of understanding of spasticity and its appropriate management. Continuity of care and knowledge, particularly across the interfaces of primary and secondary care as well as community rehabilitation teams and care agencies, is invaluable.
HYPERTONIA AND SPASTICITY
Hypertonia is the increase in tone or resistance to movement felt when a limb is passively moved. Implicit in this definition is the fact that hypertonia is determined clinically when the limb is passively moved by an examiner. As we shall see later, an increase in resistance with passive movement does not always reflect what is happening when the patient actively moves the same limb. The resistance to movement can have both viscous and elastic components. A viscous resistance is one in which the resistance increases with an increased velocity/speed of movement similar to that felt when moving a damper, such as those found attached to fire doors. An elastic resistance is one that increases with an increase in the length of the structure being moved, similar to that seen when stretching a spring. People with a high elastic resistance have high stiffness. Often the term viscoelastic resistance is used to refer to these two components that co-occur. Hypertonia can be caused by several factors1 (Figure 1.1).
• Reflexive: Here the resistance is caused by stretching the muscle, resulting in the homologous (same) muscle contracting via a stretch reflex. When the stretch reflex is enhanced, it is termed spasticity.
• Passive: This is due to the viscoelastic properties of the soft tissues (e.g. muscles and connective tissue) surrounding the joint.
• Intrinsic: This is caused by a contraction of the muscle, resulting in active formation of cross-bridges within the muscle. This could be voluntarily produced; that is, you can resist a person moving your limb by contracting your muscles. It could also be due to an involuntary contraction not caused by the stretch reflex – here, causes could be spontaneous activation of the muscle at rest (termed spastic dystonia) or an involuntary co-contraction.
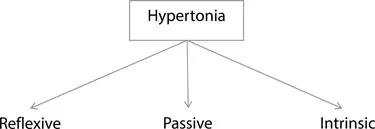
Figure 1.1 Causes of hypertonia.
In healthy subjects, stretch reflexes are only elicited with high-velocity stretches (e.g. as seen with a tendon tap using a reflex hammer that rapidly stretches the connected muscle). In these cases, the resistance felt to slow passive movement is due solely to the viscoelastic component caused by the muscle and surrounding connective tissue. In people with spasticity, stretch reflexes can be elicited at low-velocity stretches (e.g. 10°/second) meaning that an assessment of the passive, nonneural component requires even lower-velocity stretches (e.g. 5°/second).
Different conditions such as stroke, multiple sclerosis, spinal cord injury, cerebral palsy and hereditary spastic paraparesis (HSP) can show changes in both the reflexive and passive components.2,3 It is important to distinguish between the different components of hypertonia as treatment options vary – the passive component may be more amenable to physical intervention such as splinting and stretching, whilst pharmacological interventions would target the reflexive component.
SPASTICITY: DEFINITIONS AND ASSOCIATED SYMPTOMS
Spasticity may therefore be thought of as an increase in the stretch reflex size. This is in keeping with the most well-known and referenced description of spasticity proposed by Lance in 19804: ‘Spasticity is a motor disorder characterised by a velocity-dependent increase in tonic stretch reflexes (muscle tone) with exaggerated tendon jerks, resulting from hyperexcitability of the stretch reflex, as one component of the upper motor neuron syndrome’.
According to this definition, it is only the increased resistance to passive movement (muscle tone) that is defined as spasticity – other features of the upper motor neuron (UMN) syndrome, such as spasms or clonus characterised by brief, often repetitive episodes of muscle contraction, are excluded. A European working group, EU-SPASM,5 as part of a review of spasticity measurement and evaluation, has looked at this discrepancy and Lance’s definition of spasticity in detail. Three specific areas of Lance’s definition were felt to require modification:
• Velocity-dependent changes in limb stiffness during passive movement are not solely due to neural changes, but are contributed to by the normal viscoelastic properties of soft tissues (i.e. the passive component of hypertonia).6
• In addition to hyperexcitable stretch reflexes, activity in other pathways (afferent, supraspinal and changes in the α motor neuron) is also important in the development of spasticity.
• Spasticity cannot be exclusively considered a ‘motor disorder’, as afferent activity (cutaneous and proprioceptive) is also involved.
To reflect these aspects, the EU-SPASM group proposed a new definition of spasticity: ‘Spasticity – disordered sensorimotor control, resulting from an upper motor neuron lesion, presenting as intermittent or sustained involuntary activation of muscles’.
This term, although broader and consequently less specific, does now allow more aspects of the UMN syndrome to be included under the umbrella term of spasticity, such as spasms and clonus.
The UMN syndrome can be divided into so-called positive and negative aspects (Table 1.1). The positive aspects involve additional motor activity, including spasticity, spasms and clonus, while negative features include weakness, decreased postural responses and reduced dexterity. It must be remembered that these factors may occur independently of each other, but often it is the combination and interaction of the different aspects of the UMN syndrome (both positive and negative) with their functional consequences that make managing individuals so challenging. Throughout this book, the term spasticity will be used to describe the increase in muscle tone resulting from the underlying neurological condition. Other features of the UMN syndrome, such as spasms or clonus, although include...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Table of Contents
- Foreword
- Preface
- Acknowledgements
- Contributors
- PART 1 CHAPTERS
- PART 2 APPENDICES
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Spasticity Management by Valerie L. Stevenson, Louise Jarrett, Valerie L. Stevenson,Louise Jarrett in PDF and/or ePUB format, as well as other popular books in Medicine & Neurology. We have over 1.5 million books available in our catalogue for you to explore.