Many books on solution-focused brief therapy provide histories, overviews, and uses of the approach. Doing Something Different does not do any of those things. Instead, it provides those interested in the solution-focused approach with a plethora of ideas for practice, training, and simply enjoying the solution-focused approach and its practice in therapy, consulting, coaching, and training. It contains a varied and rich array of interventions, training ideas, uses with different populations and approaches, and resources written by contributors who represent many countries and viewpoints, and who are well known in the training and practice of the solution-focused approach. Chapters are presented in simple language, as befits the solution-focused approach, and complement the many serious and whimsical sections of the book, which include practice and training ideas, favorite quotes and stories, "outrageous" moments in therapy, and a list of solution-focused songs. Anyone who enjoys the approach in any manner should find something that grabs the interest and tickles the senses and sensibilities. Readers will come away informed, thoughtful, and entertained.
- 344 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Trusted by 375,005 students
Access to over 1 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
I: Interventions and Practices
1: THE OPTIMAL ZONE SCALE
Coert Visser
The scaling question is the most popular question that emerged out of the solution-focused approach. This chapter describes step-by-step how you can use the scaling question. Here is an example. Some time ago, when I was talking with a client, an interesting variation of the scaling question emerged between the two of us, which I call the “optimal zone scale.”
The woman I was coaching wanted to learn to be more assertive so that she could defend her personal boundaries and speak her mind on issues that mattered to her. This would help her to feel better at work and to keep her work load within acceptable limits. It would also help her colleagues. By being more assertive, she would be clearer to her colleagues, who would know then exactly what they could and could not expect from her. Also, she had noticed that colleagues tended to respect and value her more when she acted more assertively.
However, my client was also aware that she shouldn’t go too far in speaking her mind. She realized that if she would take this too far she could become a shrew. She absolutely did not want that. She did not want her colleagues to become afraid of her or feel intimidated. Being friendly and helpful was one of the most important aspects of her work role. So she could not afford to lose those aspects of her behavior. When she was explaining this to me I drew the picture of the scale (see Figure 1.1). The picture visualizes that there is a zone in which her behavior is effective—the optimal zone—and two zones in which it isn’t. On the left, she would be too little assertive; on the right she would be overassertive. This said, this visualization was very useful to her. She realized she was now slowly moving to the middle of the optimal zone.
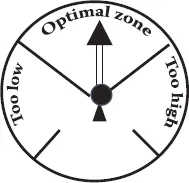
Figure 1.1 The optimal zone scale.
2: 7-ELEVEN
Frank Thomas
INSTEAD OF THE MIRACLE QUESTION
“Let’s say 6 months have passed after you finish therapy with me. We happen to run into each other at the local 7-Eleven. (Of course, I don’t walk up to you—you walk up to me, in keeping with our confidentiality agreement.) You begin to tell me how the changes you experienced during our time together have continued. What do you tell me?”
I’ve found people put themselves into a present-tense conversation quite quickly; tell me what changed; and tell me what carried over/rippled. I like it a lot—less fantasy than the miracle question, in my opinion.
3: THE SOLUTION FOCUS: A Universal Tool
Carole Waskett
Many years ago I used to live on a boat. I was married to a boat builder who restored old wooden boats. There was often no electricity in the places where Roger worked, so he had a wondrous bag of old-fashioned tools. Amongst them was a hand drill, complete with a set of augurs and other drill bits. Some of the augurs were huge like rolling pins, while some of the other drills were delicate as needles. The drill’s “mouth,” as it were, was designed to grip the end of each of the various “bits,” which Roger kept carefully wrapped in oiled leather. He and his drill were very comfortable together. It had a round wooden pad—I remember its crazed, worn surface, against which he would put pressure, to make the right-sized hole for the job in hand. He selected his bit carefully. He was so skilled that he hardly used any energy in drilling a hole. He knew just how hard to lean on the pad, holding the drill at the right angle, and turning the handle at exactly the right speed so that the resulting hole was perfect for its purpose. It was easy.
I think of the solution-focused approach (SFA) like that. With the right bit and a comfortable, experienced practitioner, it does the job sweetly and without fuss or pretension. Using the SFA, either as an assistant to someone else or as the protagonist ourselves, we use the same “handle”; we look for what’s wanted (the platform, the goal). Then we wonder what the person/group knows already: What strengths, resources, past experiences will help them to move forward? Next we look at where they are now and how they got here (scaling) or, if appropriate, we might start helping the other person/group to construct their preferred future, and then follow up with scaling.
Finally, we look at the next small concrete step. Or, rather, we elicit it; it grows, almost organically, from the preceding conversation. It needs to be articulated clearly. It may be a very small step indeed, even a recognised, quiet movement or shift somewhere in the world of the process. The bit, once it bites, winds in tiny increments into the wood, and when it begins, it is virtually inevitable that forward movement will continue.
All through, we are curious, respectful, and relaxed. We don’t try to do the tool’s job for it; we just enable it to make the most of its own superb design.
So what kinds of bits are available? We can use the approach in a wide variety of ways: Obviously, for therapy; that’s where the SFA began. Supervision follows the same path with appropriate boundaries and ethical responsibilities that maintain safety and clarity. In organisational work, we can discover where managers or teams want to go by asking questions that begin to bore into what is really wanted, and then staying behind the team (putting only gentle and appropriate pressure and encouragement on the pad) while they work out how to progress.
When we teach, we can discover and amplify the participants’ strengths and already existing knowledge of the topic; we can always provide respectful opportunities for people to express what they know and how they are thinking. As well, we can make it a habit to ask what difference the teaching session will make if it “works,” and what “work” means for this particular group. Scaling, too, is invaluable in any teaching session. Teaching is a mysterious business and needs plenty of respect, space, and air to allow learners to benefit.
These are only a few of the “bits”—the uses of the universal handle. In any situation where a preferred future and forward movement are relevant, solution-focused thinking seems to fit. I used it for myself in a tricky house move, making small steady steps in a worrying maelstrom of uncertainty, solicitors’ letters, and the movements of what to me were large sums of money. “In good order, in good heart, and moving forward,” I said to myself almost daily; the mantra was my goal at every stage, and it worked.
The wonder of the solution-focused approach is that it is strong, flexible, and reliable. Going back to the original metaphor, we need to buy a quality drill (ensure we’re well trained and educated in the model); test, experiment, and practice a lot to become quiet and comfortable with it; and select the right bit. Some practitioners develop real expertise with a particular “bit.” There are excellent therapists, for instance, who would baulk at consulting to help a team move forward in its work. Experience and success in the youth justice system may not predispose a practitioner to teaching adults.
On the other hand, some very experienced workers are confident and unfussed about working in any arena where the approach would be useful. This is often because the underlying element of the solution-focused approach—that of a respectful curiosity and the knowledge that people have the ability to progress—is in the forefront of their minds and practice. Any bit can be selected; the combination of a good reliable tool and a confident worker will get the job done.
4: SCALING AGENCY WITH CLIENTS WHEN THEY BEGIN TAKING ANTIDEPRESSANTS
Frank Thomas
A significant percentage of clients in the United States and other hard-currency countries take psychotropic medication for depression, anxiety, and other conditions. The research regarding the treatment of depression is quite clear: Those who receive both antidepressant medications and psychotherapy report greater change than those who receive only one or the other. When clients start taking antidepressants, the prescribing physician usually1 tells them about the possible negative side effects, the expected positive effects from taking the medication, and the timetable within which most patients will experience both.
One of the most common things I hear clients voice is hope that the medication will alleviate their depressive symptoms. I agree with them—who would not want clients’ problematic experiences changed for the better? However, I also take this conversation to be an opportunity to scale the person’s agency, his or her ability to choose, in order to clarify my part in the change process and the clients’ ideas about influence or control. I got this idea from Jonathan Prosser (1999, 2003), a UK psychiatrist who contributed to threads about medications and SFT on the SFT-L listserv, and from Steve de Shazer (1999), who proposed this idea on the topic of SFT and medications on the SFT-1 listserv: “Luc Isebaert’s question might be useful: ‘So, how are you going to make this medication work for you? What are you going to do to help it work?’”
THE INTERVENTION
The intervention would follow a process much like this:
Week 1
Client: Oh, I wanted to let you know that I started taking________(antidepressant) last week. I’ve been talking with my doctor. She agrees that I’m depressed, and she says this drug will help me feel better.
Therapist: OK, so you followed through with your doctor. How did you come to make that decision with her?
Client: [describes reasons for seeing the physician and process of arriving at the decision to try antidepressants]
Therapist: What did your physician say about what you could expect?
Client: [usually describes effects, negative side effects, and timetable for both]
Therapist: So… your doctor says you should feel the positive effects in 3 to 4 weeks, huh?
Client: Yes.
Therapist: And there may be negative side effects prior to seeing positive results?
Client: Yes.
Therapist: How do you see yourself coping with the negatives before you get the positives?
Follow-up questions: How else? How have you coped with negative effects outside your control in the past? What keeps your hope for change alive while you wait for the medicine to take effect?
Three weeks later
Therapist: So now that it’s been several weeks since you started taking the antidepressants, have you noticed differences?
Client: [usually discusses negative side effects and the beginning of positive effects]
Therapist: What has helped you cope with those negative effects?
Client: [usually discusses his own resources and exceptions under his control]
Therapist: OK, so you say you have coped pretty well with the negative and are finally getting some positive effects. Yet at the same time, we’ve been meeting each week for counselling and you have reported these positive changes and exceptions: (list here, with details). Many people experience even greater change in their depression (client's word) when they do “talk therapy” as well as medications. If you’re like most people, I’m wondering: How much of your positive change do you attribute to the medicine, and how much of the changes in your depression seem to respond to making changes yourself? Put it into a percentage for me, if you can—it’s just a starting point.
Client: [Invariably, the client assigns at least a small percentage to his own efforts toward change in therapy and in his daily living.]
Therapist: So, let’s just focus on that part of you and your experience that you have some control over—that part of the changes you say is not the medicine. What’s our next step regarding your depression, just in that area?
Follow-up questions: How do you see that as being under your control? How have you influenced that, on purpose? What does that say about your ability to influence part of your depression?
A Case Example
Jake and Eleanor contacted me for marriage counselling recently. Jake had suffered a heart attack 8 weeks prior to our first session, and they related that a lot of the stress that “caused”2 his heart attack came from their unhappy marriage. Unbeknownst to me, Jake had an appointment with his cardiologist between the second and third marital therapy sessions and began taking an antidepressant. When he told me, I inquired about his decision, and he informed me that he had already been experiencing the negative side effects:
Jake: You know,… .[rolls his eyes toward Eleanor]
FNT Eleanor—what’s he talking about?
Eleanor: You know… sex! [both giggle]
FNT How is it that you can both giggle about this change?
Jake: Well, now that I can’t… you know… we kiss a lot on the couch, and our 12-year-old son yells, “Ewwww! Gross!” [both laugh]
FNT: OK, how did you turn this negative side effect into something you can laugh about?
Jake: Well, we’re both committed to getting through this, and I’m just so damn hopeful for the first time in years! That’s the medication!
FNT OK, so what part of the positive changes you’ve seen so far are directly related to the medication, do you think?
Jake: [relates his elevation in mood, increased hopefulness, cessation of suicidal thoughts, and other significant changes]
FNT I couldn’t be happier for you! You didn’t mention other positive changes that you [looking at Jake] and the two [looking at Eleanor] of you tell me you’ve experienced lately. So let’s put a percentage on it, just a “guesstimate”: What percentage of the positive changes you’ve seen in your marriage would you say are related to things besides the medicine?
Eleanor: Oh, I know several [she lists three]. We were doing these even before Jake started taking the medicine.
Jake: The medicine makes it easier for me to be positive, but I’m still the one who has to act on things. [Jake describes part of his miracle morning: snuggling, inviting everyone to cook breakfast with him, listening to his son without any criti...
Table of contents
- COVER PAGE
- TITLE PAGE
- COPYRIGHT PAGE
- FOREWORD
- PREFACE
- ACKNOWLEDGMENTS
- THE EDITOR
- THE CONTRIBUTORS
- I: INTERVENTIONS AND PRACTICES
- II: TRAINING
- III: THEORY
- IV: STORIES, POEMS, SONGS, AND SOLUTION-FOCUSED QUOTES
- V: OUTRAGEOUS MOMENTS IN THERAPY
- VI: RESOURCES
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Doing Something Different by Thorana S. Nelson in PDF and/or ePUB format, as well as other popular books in Psychology & Education in Psychology. We have over one million books available in our catalogue for you to explore.