- 336 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Managing Allergens in Food
About this book
Controlling allergens in food is a matter of increasing importance for the food industry, especially in light of recent legislation. Effective handling of allergens depends on identifying allergenic ingredients, creating separate production lines for allergen-free products, and effective labelling to inform consumers about which products are safe to eat. Recent attention has also focused on novel methods to manage allergens in food, for example by reducing allergenicity through the prudent selection of raw food materials and improved processing techniques. This important collection provides a clear introduction to food allergens and allergy and offers a comprehensive review of current research contributing to safer food production with regard to allergens.Part one discusses the diagnosis of offending foods and how allergens can affect the quality of life. Expanding on these fundamentals, part two reviews the effect of different methods of food processing on allergens and novel technologies which can reduce the potency of allergens or remove them altogether from foods. The final part of the book covers the key area of risk assessment and allergen management to achieve more uniform standards within the industry. Practical strategies to improve consumer acceptance of GM foods are also discussed.With its distinguished editors and array of international contributors, Managing allergens in food is an essential reference for producers, manufacturers, retailers and all those wishing to improve safety in the food industry.
- Presents a cohesive summary of recent research into safer food production
- Discusses the effects of food processing on allergens
- An international team of editors
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Part I
What are food allergens and allergies?
1
Food allergy: current diagnosis and management
M. Fernández-Rivas, Hospital Clínico San Carlos, Spain
B. Ballmer-Weber, University Hospital of Zurich, Switzerland
Publisher Summary
The term adverse reaction to food applies to any clinically abnormal response induced by a food (or a food additive). It comprises a wide spectrum of clinical entities with different pathomechanisms, diagnostic procedures, and therapeutic options. The European Academy of Allergology and Clinical Immunology (EAACI) proposed a classification of adverse reactions to food based on mechanisms, which is shown and discussed in this chapter. Adverse reactions to food can be divided into toxic and non-toxic reactions. Toxic reactions depend on the food itself and will occur in any exposed individual provided that the dose is high enough. Non-toxic reactions depend on the individual susceptibility to the food and can be classified into immune-mediated or non-immune-mediated. Immune-mediated reactions can be further divided into IgE and non-IgE-mediated reactions. The role of type I, IgE-mediated reactions has been well established and proven to be causative of clinical symptoms by Double-Blind, Placebo-Controlled Food Challenge (DBPCFC). Non-immune-mediated adverse reactions comprise different clinical conditions divided into enzymatic (enzyme deficiencies), pharmacologic or undefined. The chapter focuses on the IgE-mediated allergic reactions induced by the food ingestion.
1.1 Introduction: key definitions
1.1.1 Nomenclature
The term adverse reaction to food applies to any clinically abnormal response induced by a food (or a food additive). It comprises a wide spectrum of clinical entities with different pathomechanisms, diagnostic procedures and therapeutic options. The European Academy of Allergology and Clinical Immunology (EAACI)1 proposed a classification of adverse reactions to food based on mechanisms, which is shown in Fig. 1.1 and discussed below.

Adverse reactions to food can be divided into toxic and non-toxic reactions. Toxic reactions depend on the food itself and will occur in any exposed individual provided that the dose is high enough. Non-toxic reactions depend on the individual susceptibility to the food, and can be classified into immune-mediated or non-immune-mediated. Immune-mediated reactions can be further divided into IgE and non-IgE-mediated reactions. The role of type I, IgE-mediated reactions has been well established and proven to be causative of clinical symptoms by double-blind, placebo-controlled food challenge (DBPCFC). Non-immune-mediated adverse reactions comprise different clinical conditions divided into enzymatic (enzyme deficiencies), pharmacologic (e.g. vasoactive amines present in foods) or undefined.
Some differences exist between the nomenclature of adverse reactions to food used in Europe1,2 and in the USA,3 as it is shown in Fig. 1.1. This chapter will deal with IgE-mediated allergic reactions induced by the food ingestion. Foods can also elicit IgE-mediated reactions through skin contact or inhalation, but they will not be reviewed.
1.1.2 Epidemiology
The general population perceives food allergy as a major health problem, although only a minority of the claims can be confirmed after a full clinical evaluation including controlled oral challenges. There is also the perception that the prevalence and severity of food allergy are increasing, which seems actually the case for peanut allergy.4–6 Recent population surveys have provided some insight into the prevalence of food allergy.7–17 As is shown in Table 1.1, food allergy affects 1% to 3% of the general population, and is more frequent in children, especially under 3 years of age in whom the prevalence of food allergy may be up to 8%. However, differences in study design and diagnostic criteria render comparisons between studies difficult. Large international epidemiological studies on food allergy, including an objective diagnosis by means of IgE tests and DBPCFC, will provide comparable point prevalences and will allow us to study the contribution of population-related factors.
Table 1.1
Prevalence of food allergy
| Country | Sample | Reported prevalence | Confirmed prevalence (IgE tests, DBPCFC) | Reference |
| United Kingdom | 7500 households | 20% | 1.4%–1.8% | Young 19947 |
| The Netherlands | 1483 adults | 12.4% | 2.4% | Jansen, 19948 |
| 15 countries | 17 280 adults | Mean 12% | No | Woods, 20019 |
| ECRHS | (20–44 y) | Range: 4.6% in Spain – 19.1% in Australia | ||
| France | 33 110 individuals (all age groups) | 3.24% | No | Kanny, 200110 |
| Germany | 13 300 individuals (all age groups) | 34.9% | 2.5% | Zuberbier, 200411 |
| Finland | 866 children (1–6 y) | 23% | 8% | Kajosaari, 198212 |
| USA | 480 children (1–3 y) | 28% | 8% | Bock, 198713 |
| Sweden, | 652 children | 27% | 2% | Kristjansson, 199914 |
| Iceland | (18 m) | 28% | 2% | |
| Germany | 2354 children (0–17 y) | 38.4% | 3.5% | Roehr, 200415 |
| Denmark | 898 children | 13.03% | 2.3% in 3 y | Osterballe, 200516 |
| 936 adults | 1% in children >3 y | |||
| 3.2% in adults | ||||
| United Kingdom | 757 children of 11 y | 11.6% | 2.3% | Pereira, 200517 |
| 775 children of 15 y | 12.4% | 2.3% |
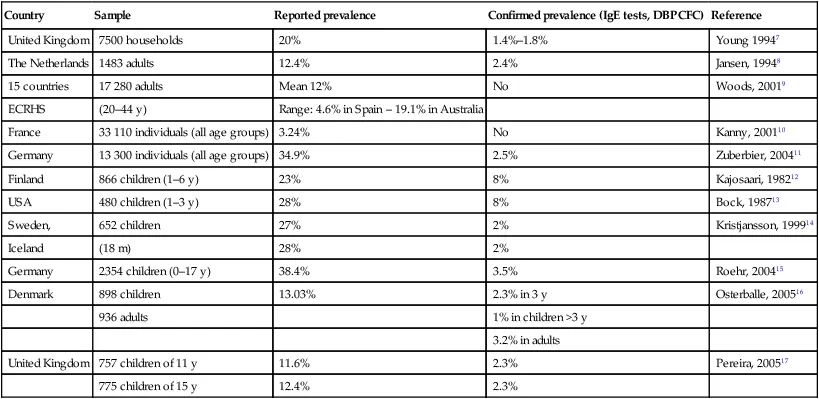
ECRHS, European Community Respiratory Health Survey; y, years; m, months.
The prevalence of food allergy is higher in patients with atopic diseases and especially in children with atopic dermatitis. Approximately one-third of children with mild to moderate atopic dermatitis have a food allergy.18,19 Atopy is an important risk factor in those food allergies arising in early infancy. Indeed, food allergy seems to start the ‘allergic march’ from atopic dermatitis to allergic rhinitis and asthma. This is supported by the finding that food allergy in infancy, and especially egg allergy, is associated with increased aeroallergen sensitisation and increased allergic rhinitis and asthma in childhood.19–21
1.2 Offending foods
The foods most frequently involved in allergic reactions are cow’s milk, hen’s egg, peanut and tree nuts, fish, shellfish, soya, fruits and legumes. The relative importance of these foods varies widely with the age of the patients and the geographical location. Cow’s milk and eggs are the most prevalent food allergies in infants and children in all series, as a consequence of the worldwide consumption of these foods in this age group. Local differences in the prevalence of some specific foods are well known, i.e. peanut allergy is frequently observed in early childhood in the USA, allergy to fish is common in Spain and Japan, sesame allergy in Israel, and mustard allergy in France.4,5,10–17, 22–26 Altogether, these studies suggest that, when the sensitisation is produced through the oral route (in the so-called ‘class I food allergy’27), the timing of exposure, and the dietary habits play a significant role in determining the prevalence of specific food allergies.
The overall prevalence of food allergy and the prevalence of allergies to specific foods change from children to adults due (in part) to the development of oral tolerance for some foods. In a Danish cohort of 1749 newborns followed for 15 years, the prognosis of cow’s milk allergy/intolerance was good with a total recovery of 56% at 1 year, 87% at 3 years and 97% at 15 years.28 Egg allergy is often lost over time as well, and fish allergy may be outgrown, although to a lesser ext...
Table of contents
- Cover image
- Title page
- Table of Contents
- Related titles
- Copyright
- Contributor contact details
- Preface
- Part I: What are food allergens and allergies?
- Part II: Allergens in foods - from raw to processed foods
- Part III: Assessing allergic risks and practical management of allergens in food
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Managing Allergens in Food by Clare Mills,Harry Wichers,Karin Hoffmann-Sommergruber in PDF and/or ePUB format, as well as other popular books in Technology & Engineering & Food Science. We have over 1.5 million books available in our catalogue for you to explore.