eBook - ePub
Self Assessment in Musculoskeletal Pathology X-rays
This is a test
Buch teilen
- 290 Seiten
- English
- ePUB (handyfreundlich)
- Über iOS und Android verfügbar
eBook - ePub
Self Assessment in Musculoskeletal Pathology X-rays
Angaben zum Buch
Buchvorschau
Inhaltsverzeichnis
Quellenangaben
Häufig gestellte Fragen
Wie kann ich mein Abo kündigen?
Gehe einfach zum Kontobereich in den Einstellungen und klicke auf „Abo kündigen“ – ganz einfach. Nachdem du gekündigt hast, bleibt deine Mitgliedschaft für den verbleibenden Abozeitraum, den du bereits bezahlt hast, aktiv. Mehr Informationen hier.
(Wie) Kann ich Bücher herunterladen?
Derzeit stehen all unsere auf Mobilgeräte reagierenden ePub-Bücher zum Download über die App zur Verfügung. Die meisten unserer PDFs stehen ebenfalls zum Download bereit; wir arbeiten daran, auch die übrigen PDFs zum Download anzubieten, bei denen dies aktuell noch nicht möglich ist. Weitere Informationen hier.
Welcher Unterschied besteht bei den Preisen zwischen den Aboplänen?
Mit beiden Aboplänen erhältst du vollen Zugang zur Bibliothek und allen Funktionen von Perlego. Die einzigen Unterschiede bestehen im Preis und dem Abozeitraum: Mit dem Jahresabo sparst du auf 12 Monate gerechnet im Vergleich zum Monatsabo rund 30 %.
Was ist Perlego?
Wir sind ein Online-Abodienst für Lehrbücher, bei dem du für weniger als den Preis eines einzelnen Buches pro Monat Zugang zu einer ganzen Online-Bibliothek erhältst. Mit über 1 Million Büchern zu über 1.000 verschiedenen Themen haben wir bestimmt alles, was du brauchst! Weitere Informationen hier.
Unterstützt Perlego Text-zu-Sprache?
Achte auf das Symbol zum Vorlesen in deinem nächsten Buch, um zu sehen, ob du es dir auch anhören kannst. Bei diesem Tool wird dir Text laut vorgelesen, wobei der Text beim Vorlesen auch grafisch hervorgehoben wird. Du kannst das Vorlesen jederzeit anhalten, beschleunigen und verlangsamen. Weitere Informationen hier.
Ist Self Assessment in Musculoskeletal Pathology X-rays als Online-PDF/ePub verfügbar?
Ja, du hast Zugang zu Self Assessment in Musculoskeletal Pathology X-rays von im PDF- und/oder ePub-Format sowie zu anderen beliebten Büchern aus Medicine & Orthopedics. Aus unserem Katalog stehen dir über 1 Million Bücher zur Verfügung.
Information
Thema
MedicineThema
Orthopedics1
Arthritis
Karen Sakthivel-Wainford
Introduction
Arthritis is a collection of diseases that affect the true or diarthrodial joint (see Figure 1.1). A diarthrodial joint consists of cartilage covering the articular ends of the bones forming the joints, the articular capsule which is reinforced by ligamentous structures and the joint space which is lined with synovial membrane and filled with synovial fluid.
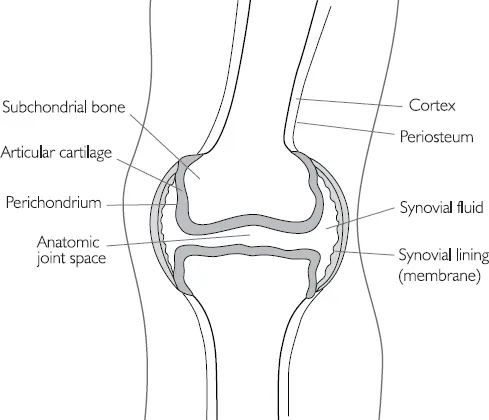
Figure 1.1 Diarthrodial joint
The abnormality of the joint in arthritis usually consists of destruction of the articular cartilage which appears on the radiograph as a narrowing of the joint space; narrowing of the joint is the cardinal sign of arthritis. However in some arthritic processes the joint space may become expanded instead, for example in the early stages of some arthrides, when there is joint effusion and ligament laxity.
However this does not help in distinguishing one arthropathy from another radiographically. The rest of this chapter will give brief descriptions of some of the most common arthropathies, but mainly will attempt to give some guidance in distinguishing one arthropathy from another.
In order to focus our minds when looking at arthrides, Debbie Forrester (Forrester and Brown, 1998) suggests the following ABCS search pattern:
Alignment (is there subluxation or dislocation?)Bone mineralisation (is sclerosis or osteopenia present?)Cartilage (including a search for erosions, plus loss of joint space)Soft tissues (is there soft tissue swelling, tophi of gout, calcification in the soft tissues as in scleroderma?)
Helms (1995) expands on this by including D for distribution, making it ABCDS. For example, in the hands what is the distribution of the disease process? Is it distal (as in osteoarthritis), or proximal (as in rheumatoid arthritis)? Also does the distribution affect the spine, or the sacroiliac joints? According to Helm if the distribution can be determined the differential diagnosis can become quite short. However sometimes in the hands it can be difficult to assess the distribution, particularly when there is severe rheumatoid arthritis and the proximal nature of disease is not evident.
Below are some of the many arthropathies, for which I will give some key points in their radiographic appearance, in order to help you recognise them. Radiographic examples of arthropathies and more information will be found in the case studies.
Arthrides and Arthropathies
Osteoarthritis
Diffuse idiopathic skeletal hyperostosis
Inflammatory arthritis
• Rheumatoid arthritis
Rheumatoid variants:
• Ankylosing spondylitis
• Reiter’s syndrome
• Psoriatic arthritis
Metabolic and endocrine:
• Calcium pyrophosphate disease
• Gout
Charcot joint
Connective tissue arthropathy:
• Systemic lupus erythematosus
• Scleroderma
• Dermatomyositis
Synovial osteochondromatosis
Infectious arthritis
Osteoarthritis
Osteoarthritis (OA) is the commonest chronic joint disease, characterised by the progressive erosion of articular cartilage. The association between OA and aging is well documented but is in fact non-linear; the prevalence increases exponentially over the age of 50 years. About 80% to 90% of individuals of both sexes have evidence of OA by the time they reach 65 years of age.
In the majority of instances OA appears insidiously, without apparent initiating cause as an aging phenomenon (idiopathic or primary OA). In these cases, the disease is usually oligoarticular but may be generalised. In about 5% of cases OA may appear in younger individuals with some predisposing conditions, such as previous macro trauma or repeated micro trauma to a joint, a congenital development deformity of a joint, or some underlying systemic disease such as diabetes, haemochromatous or marked obesity. In these cases the disease is called secondary OA and often involves one or several predisposed joints. OA is sometimes referred to as degenerative joint disease.
Gender has some influence on distribution, for example, the knees and hands are more commonly affected in women and hips in men. Primary general OA sometimes with familial influence is more common in women. Primary OA is seen only in the hands, where it affects the distal interphalangeal joints, the proximal interphalangeal joints and the base of the thumb in a bilateral symmetrical way.
The radiographic hallmarks of OA are:
• sclerosis
• osteophytes
• joint space narrowing
• distal distribution in the hands.
Joint space narrowing is the least specific (as mentioned earlier), but is always present in OA. Subchondral sclerosis is always present unless severe osteoporosis is present, which causes sclerosis to be diminished; osteophytosis may also be diminished in the presence of osteoporosis.
Another type of OA, although relatively rare, is erosive OA. It tends to be very painful and debilitating with identical distribution to primary OA (it affects the hands, the distal interphalangeal joints, proximal interphalangeal joints and the base of the thumb), but it is associated with severe osteoporosis and erosions of the hands.
Several other joints may demonstrate erosions as part of OA changes:
• temporomandibular joints
• sacroiliac joints
• acromioclavicular joints
• symphysis pubis.
Subchondral cysts or geodes may also be seen in OA, often in the shoulder or hip. In the hip they are sometimes called Edgars’ cysts.
Pathology
In the early stages of OA the chondrocytes proliferate forming ‘clones’. This is accompanied by biochemical changes as the water content of the matrix increases and the concentration of proteoglycins from the superficial zone of articular cartilage decreases. Disruption of the smooth surface of cartilage follows; parallel collagen fibres initially become tangential to the surface (flaking) and then extend vertically into the deeper zones (fibrillation) and cracking of the matrix occurs.
Gross examination at this stage would reveal a granular articular surface that is softer than normal. Friction smoothes the exposed bone, giving it the appearance of polished ivory (bone eburnation). At the same time there is thickening of the subchondral bone plate, rebuttressing and sclerosis of the underlying cancellous bone. Small fractures of the articulating bone are common and the dislodged pieces of cartilage and subchondral bone fall into the joint forming loose bodies (joint mice). The gaps at these fracture sites allow synovial fluid to be forced into the subchondral region in a one-way, ball-valve like mechanism. The loculated fluid collection increases in size, forming fibrous walled cysts. Mushroom shaped osteophytes develop at the margins of the articular surface and are capped by fibrocartilage and hyaline cartilage that gradually ossifies. See Figure 1.2.
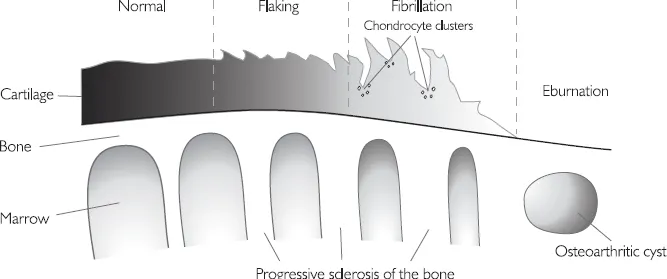
Figure 1.2 A schematic representation of the sequential changes of osteoarthritis
Diffuse idiopathic skeletal hyperostosis (DISH)
DISH is the only disease that causes osteophytes without loss of joint space, or sclerosis. It is of unknown aetiology. It results in severe productive changes of the spine, including annulus fibrosus, anterior longitudinal ligament, and sometimes paravertebral connective tissue.
Three criteria exist for diagnosis:
• flowing ossification of the anterolateral aspect of at least four continuous vertebral bodies
• preservation of disc height
• sacroiliitis and facet joint ankylosis are not present.
Inflammatory Arthritis
Rheumatoid Arthritis
Rheumatoid arthritis (RA) is a common arthritis of unknown aetiology which causes synovial inflammation and articular destruction that is often polyarticular. The term ‘classic RA’ is used to refer to one form of arthritis of unknown aetiology, other forms being considered a variant of this standard type. Classic RA may be described as follows: the patient is a young adult, more often female, complaining of pains in many joints, particularly fingers, wrists, elbows, knees and ankles. The same joints are affected in both limbs, though not necessarily with equal severity. Patients with classical RA normally have signs of an inflammatory, erosive arthritis and a positive rheumatoid factor. See Figure 1.3.
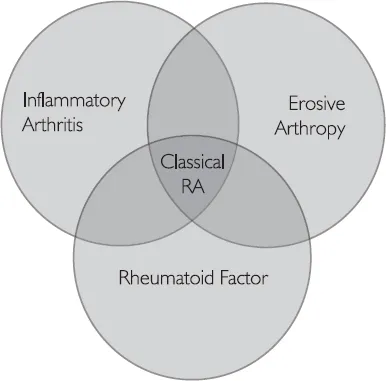
Figure 1.3 Venn diagram of classic RA
RA radiographic hallmarks are:
• soft tissue swelling
• osteoporosis
• joint space narrowing
• marginal erosions
• proximal and bilateral symmetry in the hands (unless the patient has had a stroke, in which case the affected side is spared).
Table 1.1 ...