
eBook - ePub
Clinical Handbook of Interstitial Lung Disease
Keith C. Meyer, Muhunthan Thillai, David R. Moller, Muhunthan Thillai, David R. Moller, Keith C. Meyer
This is a test
Buch teilen
- 529 Seiten
- English
- ePUB (handyfreundlich)
- Über iOS und Android verfügbar
eBook - ePub
Clinical Handbook of Interstitial Lung Disease
Keith C. Meyer, Muhunthan Thillai, David R. Moller, Muhunthan Thillai, David R. Moller, Keith C. Meyer
Angaben zum Buch
Buchvorschau
Inhaltsverzeichnis
Quellenangaben
Über dieses Buch
This handbook provides clinical guidance to the practicing physician on the diagnosis and treatment of Interstitial Lung Diseases (ILD). A contributed work with invited chapters which draw on the knowledge and experience of recognised global leaders in respiratory medicine, it is authoritative, concise and portable and is intended for use in a fast-paced clinical setting. The book:
- offers practical tips and clear guidance for clinicians
-
- provides detailed explanations of the main therapeutic options for each individual ILD
-
- contains high-quality visuals, including radiology and histopathology of the most common as well as some of the rarer ILDs
-
- discusses individual ILDs and has topics common to all including critical care, lung transplantation and palliative care
-
- navigates clinicians through cases with decision making guidelines and algorithms
-
- includes appendices with international practice guidelines, sample patient information sheets and other helpful resources.
-
Emphasizing how to perform a thorough assessment of an ILD patient for accurate diagnosis and their subsequent effective management, this is both a gold standard text as well as a daily companion for physicians caring for ILD patients. A first-of-its-kind, it will become the go-to guide for all clinicians who manage patients with ILD.
Häufig gestellte Fragen
Wie kann ich mein Abo kündigen?
Gehe einfach zum Kontobereich in den Einstellungen und klicke auf „Abo kündigen“ – ganz einfach. Nachdem du gekündigt hast, bleibt deine Mitgliedschaft für den verbleibenden Abozeitraum, den du bereits bezahlt hast, aktiv. Mehr Informationen hier.
(Wie) Kann ich Bücher herunterladen?
Derzeit stehen all unsere auf Mobilgeräte reagierenden ePub-Bücher zum Download über die App zur Verfügung. Die meisten unserer PDFs stehen ebenfalls zum Download bereit; wir arbeiten daran, auch die übrigen PDFs zum Download anzubieten, bei denen dies aktuell noch nicht möglich ist. Weitere Informationen hier.
Welcher Unterschied besteht bei den Preisen zwischen den Aboplänen?
Mit beiden Aboplänen erhältst du vollen Zugang zur Bibliothek und allen Funktionen von Perlego. Die einzigen Unterschiede bestehen im Preis und dem Abozeitraum: Mit dem Jahresabo sparst du auf 12 Monate gerechnet im Vergleich zum Monatsabo rund 30 %.
Was ist Perlego?
Wir sind ein Online-Abodienst für Lehrbücher, bei dem du für weniger als den Preis eines einzelnen Buches pro Monat Zugang zu einer ganzen Online-Bibliothek erhältst. Mit über 1 Million Büchern zu über 1.000 verschiedenen Themen haben wir bestimmt alles, was du brauchst! Weitere Informationen hier.
Unterstützt Perlego Text-zu-Sprache?
Achte auf das Symbol zum Vorlesen in deinem nächsten Buch, um zu sehen, ob du es dir auch anhören kannst. Bei diesem Tool wird dir Text laut vorgelesen, wobei der Text beim Vorlesen auch grafisch hervorgehoben wird. Du kannst das Vorlesen jederzeit anhalten, beschleunigen und verlangsamen. Weitere Informationen hier.
Ist Clinical Handbook of Interstitial Lung Disease als Online-PDF/ePub verfügbar?
Ja, du hast Zugang zu Clinical Handbook of Interstitial Lung Disease von Keith C. Meyer, Muhunthan Thillai, David R. Moller, Muhunthan Thillai, David R. Moller, Keith C. Meyer im PDF- und/oder ePub-Format sowie zu anderen beliebten Büchern aus Medizin & Lungenheilkunde & Thoraxmedizin. Aus unserem Katalog stehen dir über 1 Million Bücher zur Verfügung.
Information
1
An overview of the classification and diagnosis of interstitial lung disease
Keith C Meyer
Historical background and evolution of terminology
Current classification systems for ILD
Idiopathic interstitial pneumonias
Genetics of ILD: Potential impact on classification and terminology
Current approach to making a confident ILD diagnosis
Summary
References
Historical background and evolution of terminology
Recognition of the existence of interstitial lung disease (ILD) dates back more than 100 years when Sir William Osler described ‘cirrhosis of the lungs’ and recognized the diversity of its forms and the difficulty of classifying these disorders (1). Various terminologies were coined over the span of the twentieth century as various leaders in the field described patients whose lungs displayed changes of interstitial inflammation and fibrosis. Hamman and Rich (1944) described four cases of rapidly progressive, diffuse alveolar wall thickening without identifiable cause, which led to use of the term, ‘Hamman–Rich syndrome’ for either acute-onset or chronic fibrotic ILD. Subsequently, diffuse pulmonary fibrosis was linked to forms of connective tissue disease (CTD) and other causes, such as exposure to organic or inorganic dusts and pneumotoxic drug reactions, but many forms remained unexplained by any associations. Terms such as ‘chronic idiopathic interstitial fibrosis’, ‘diffuse fibrosing alveolitis’ or ‘idiopathic pulmonary fibrosis’ were used to designate fibrotic ILD of unknown aetiology, and these disorders were thought to occur as a consequence of alveolar wall inflammation (‘alveolitis’). The term ‘diffuse fibrosing alveolitis’ was coined by Scadding (2) to describe widespread fibrotic change beyond the level of the terminal bronchioles, and Scadding subdivided entities according to known or unknown associations and patterns of fibrosis (Figure 1.1). Liebow and Carrington (3,4) published a classification system for chronic idiopathic interstitial pneumonias that was based on histopathologic changes; one of the five subgroups that they described was termed ‘usual’ interstitial pneumonia (UIP), and the Hamman–Rich syndrome was felt to be an acute form of UIP (Figure 1.1).
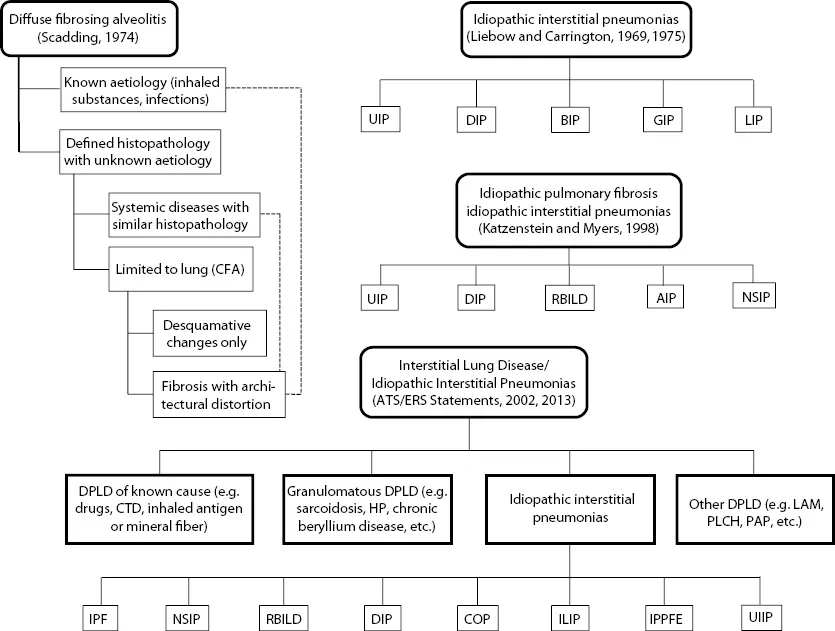
Figure 1.1Evolution of classification systems for interstitial lung disease and forms of idiopathic interstitial pneumonia. (Abbreviations: AIP = acute interstitial pneumonia; BIP = bronchiolitis interstitial pneumonia; CFA = cryptogenic fibrosing alveolitis; COP = cryptogenic organizing pneumonia; CTD = connective tissue disease; DIP = desquamative interstitial pneumonia; DPLD = diffuse parenchymal lung disease; GIP = giant cell interstitial pneumonia; HP = hypersensitivity pneumonia; ILIP = idiopathic lymphoid interstitial pneumonia; IPF = idiopathic pulmonary fibrosis; IPPFE = idiopathic pleuropulmonary fibrosis; LAM = lymphangioleiomyomatosis; NSIP = non-specific interstitial pneumonia; PLCH = pulmonary Langerhans cell histiocytosis; RBILD = respiratory bronchiolitis interstitial lung disease; UIIP = undifferentiated interstitial pneumonia; UIP = usual interstitial pneumonia.)
The classification systems proposed by Scadding or Liebow and Carrington were quite similar, but clinicians tended to overlook histopathologic variations and termed ‘chronic idiopathic fibrosing ILD’ as ‘cryptogenic fibrosing alveolitis’ (Europeans) or ‘idiopathic pulmonary fibrosis’ (United States). Katzenstein and Myers (5) re-examined Liebow’s classification system and refined the histopathology-based system by adding two new categories (non-specific interstitial pneumonia [NSIP] and respiratory-bronchiolitis-associated ILD [RBILD]) while revising/retaining some of Liebow’s categories (UIP and desquamative interstitial pneumonia [DIP]): acute interstitial pneumonia (AIP) was coined as a term for the Hamman–Rich syndrome (Figure 1.1). Their scheme recognized giant cell interstitial pneumonia (GIP) as caused by hard-metal exposure and considered lymphoid interstitial pneumonia (LIP) as a lymphoproliferative disorder, while bronchiolitis interstitial pneumonia (BIP) was recognized as an intraluminal (rather than interstitial) process that could take the form of organizing pneumonia (aka bronchiolitis obliterans organizing pneumonia [BOOP]) or diffuse alveolar damage (DAD). They also correlated their histopathologic pattern-based classification system with clinical features and natural history.
With the evolution of ongoing clinical and pathologic investigations of ILD from the late twenti...