![]()
Integrating IMRT and IGRT into Treatment Delivery
Meyer JL (ed): IMRT, IGRT, SBRT - Advances in the Treatment Planning and Delivery of
Radiotherapy, ed 2, rev. and ext. Front Radiat Ther Oncol. Basel, Karger, 2011, vol. 43, pp 132–164
______________________
Technologies of Image Guidance and the Development of Advanced Linear Accelerator Systems for Radiotherapy
Vincent W.C. Wuc • Maria Y.Y. Lawc • Josh Star-Lackb • Fion W.K. Cheungc,d • C. Clifton Ling a-c
aDepartment of Medical Physics, Memorial Sloan-Kettering Cancer Center, New York, N.Y., bVarian Medical Systems, Palo Alto, Calif., USA; cDepartment of Health Technology and Informatics, Hong Kong Polytechnic University, and d Department of Clinical Oncology, Queen Elizabeth Hospital, Hong Kong, China
______________________
Abstract
As advanced radiotherapy approaches for targeting the tumor and sparing the normal tissues have been developed, the image guidance of therapy has become essential to directing and confirming treatment accuracy. To approach these goals, image guidance devices now include kV on-board imagers, kV/MV cone-beam CT systems, CT-on-rails, and mobile and in-room radiographic/fluoroscopic systems. Nonionizing sources, such as ultrasound and optical systems, and electromagnetic devices have been introduced to monitor or track the patient and/or tumor positions during treatment. In addition, devices have been designed specifically for monitoring and/or controlling respiratory motion. Optimally, image-guided radiation therapy systems should possess 3 essential elements: (1) 3D imaging of soft tissues and tumors, (2) efficient acquisition and comparison of the 3D images, and (3) an efficacious process for clinically meaningful intervention. Understanding and using these tools effectively is central to current radiotherapy practice. The implementation and integration of these devices continue to carry practical challenges, which emphasize the need for further development of the technologies and their clinical applications.
Copyright © 2011 S. Karger AG, Basel
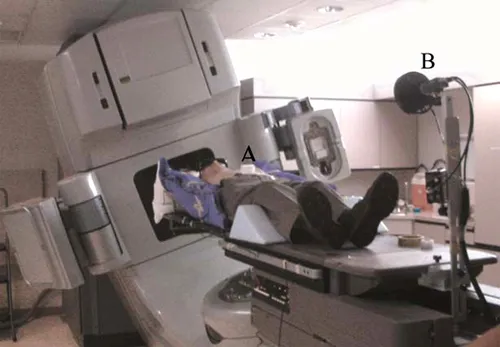
The evolution of technologies for image-guided radiation therapy (IGRT) has been rapid over the last 2 decades. During the 1980s, computer control of the linear accelerator (linac) was implemented, which was an important step for subsequent developments. Subsequently, electronic portal imaging devices (fig. 1) were introduced, enabling digital portal imaging - the first step in modern IGRT. More recently, imaging devices capable of generating 3D images of soft tissues have been incorporated into radiation treatment devices, ushering in a new era of IGRT [1]. Of course, image guidance (IG) for radiation oncology has broader meanings [2], and perhaps the current process should really be called IG during radiation treatment delivery. In the past decade, we have seen a plethora of other IG devices such as kV on-board imagers, kV/MV cone-beam CT (CBCT) systems, CT-on-rails, and mobile and in-room radiographic/fluoroscopic systems. Nonionizing sources, such as ultrasound and optical systems, and electromagnetic devices, were introduced to set up, monitor, or track the patient and/or tumor positions during treatment. In addition, devices were designed specifically for monitoring and/or controlling respiratory motion [e.g. the Varian Real-Time Position Management (RPM) System; fig. 2].
Fig. 1. Linear accelerator equipped with electronic portal imaging device.
Since many of these systems serve different functions, well-equipped facilities may have a multitude of such devices, each serving a specific function but not interfacing well with the other devices, or even with the linac. The delivery process may be much less seamlessly integrated. In addition, each new device arrives with a dedicated computer, requiring its own interfaces, networks and workarounds for practical implementation. As shown in figure 3, the control area of a radiation therapy machine can become crowded with computer monitors, increasing the burden and complexities confronted by the radiotherapists and staff.
Fig. 2. RPM system by Varian Medical Systems: infrared reflector (A), infrared camera (B).
Fig. 3. The display workstations in the control room of a linear accelerator. Each workstation displays one function during treatment delivery.
Technologies to Meet the Goals of Image-Guided Radiation Therapy
The goal of IGRT is to reduce treatment uncertainties, which can occur between fractions (interfraction) or during the treatment (intrafraction). Imaging can provide guidance of treatment in several ways. To address interfractional errors, repositioning or replanning can be performed. To reduce intrafractional uncertainties, imaging during treatment can monitor the positions of internal structures and provide the basis for correction. In developing technologies for IGRT, the key issues are whether the imaging systems and processes are efficient and accurate enough. Ling et al. [1] and Greco and Ling [2], suggested that an ideal IGRT system should possess 3 essential elements: (1) 3D imaging of soft tissues and tumors, (2) efficient acquisition and comparison of the 3D images, and (3) an efficacious process for clinically meaningful intervention.
Huntzinger et al. [3] described 4 technical criteria for the assessment of successful technologies for image-guided stereotactic radiosurgery: (1) a treatment planning system that generates dose distributions, with rapid dose fall-off from the tumor in all 3 dimensions, through the use of beams converging from many directions; (2) imaging systems with submillimeter accuracy that can account for target motion; (3) a high-resolution, accurate and efficient delivery method; and (4) a system that is fully integrated to enable perfect geometric alignment between imaging, planning and targeting of tumor volumes.
Others have commented on the cost-benefit analysis of the new technologies [1, 4, 5]. In terms of economics, there is significant cost in initiating and implementing IGRT. Other than the investment in the in-room imaging and motion control facilities, human resources and machine time are also important considerations. The increased machine time per patient means an overall reduced throughput of patients per machine. Questions can be raised if the increased cost is not balanced by the benefits that IGRT will bring.
If our goal is to improve clinical outcomes in a cost-effective manner, then a major challenge becomes how to best apply the various technologies that have been developed. The addition of new, emerging technologies will only intensify this concern. For simplicity, perhaps we can consider 2 steps in meeting this challenge. The first is a vetting process in terms of what individual devices will be used, when to use them and how to use them. The second is how best to integrate the selected devices, systems and processes with linac-based radiation delivery in a coordinated approach.
Validation and Vetting of Image-Guided Radiation Therapy Devices
Ideally, the evaluation of the clinical efficacy of a technology should involve the quantification of its benefits in objective clinical outcome measures. To be reliable, this requires comparative phase III clinical trials with sufficient follow-up. There are many obstacles for such trials. The time required for their planning, approval and organization, reticence to submit cases to the randomization process, and clinical imperatives to individualize treatments based on the specifics of medical cases lead to difficulties in patient accrual and render such trials highly impractical. Even if conducted, due to the lengthy nature of clinical trials and the rapid evolution of the technologies, the conclusions may be outdated and irrelevant before they are even derived [4, 5]. A recent perusal of a database on IGRT publications revealed little data reporting objective clinical outcomes.
In the absence of clinical outcome data, we are left with surrogates for documenting clinical advances. This approach retreats to the dogma that reductions of setup uncertainties and minimizations of organ motion effects, carefully measured, lead to outcome improvements. Even with these data, there will be many challenges in the vetting process of devices. This is partly because there are many competing and an ever increasing variety of technologies and products, and partly because the standards and metrics for their evaluation are still evolving. Some of the metrics may be easy to define, such as spatial accuracy, acquisition time, invasiveness and soft tissue contrast/discrimination. Others are more nebulous, with some being device-specific and/or institution-specific in terms of the usefulness of an approach. The surrogates and metrics used in various studies on IGRT will be described in more detail in later sections.
Other factors in the evaluation of a device or system are its applicability and ease of use. In general, devices that can be applied to many major disease sites will be more widely accepted. As to ease of use, Joel Tepper recently said ‘the less direct physician physical intervention, the more likely newer techniques will be accepted’, highlighting the importance of physicians’ acceptance of their involvement in the workflow of IGRT. This precept could be broadened to ‘the less direct user (clinicians, physicists and radiotherapists) physical intervention, the more likely newer techniques will be accepted’.
The ease of use of a device also depends on how well it is integrated into the treatment pro...