Respiratory Medicine Lecture Notes covers everything from the basics of anatomy and physiology, through to the aetiology, epidemiology, symptoms and management of a full range of respiratory diseases, providing a comprehensive yet easy-to-read overview of all the essentials of respiratory medicine. Key features of this new, full-colouredition include: •Updated and expanded material on chest X-rays and radiology •Self-assessment exercises for each chapter •A range of clinical images and scans showing the key features of each disease •Fully supported by a companion website at www.lecturenoteseries.com/respiratory featuring figures, key points, web links, and interactive self-assessment questions Ideal for learning the basics of the respiratory system, starting a placement, or as a quick-reference revision guide, Respiratory Medicine Lecture Notes is an invaluable resource for medical students, respiratory nurses and junior doctors.
Häufig gestellte Fragen
Wie kann ich mein Abo kündigen?
Gehe einfach zum Kontobereich in den Einstellungen und klicke auf „Abo kündigen“ – ganz einfach. Nachdem du gekündigt hast, bleibt deine Mitgliedschaft für den verbleibenden Abozeitraum, den du bereits bezahlt hast, aktiv. Mehr Informationen hier.
(Wie) Kann ich Bücher herunterladen?
Derzeit stehen all unsere auf Mobilgeräte reagierenden ePub-Bücher zum Download über die App zur Verfügung. Die meisten unserer PDFs stehen ebenfalls zum Download bereit; wir arbeiten daran, auch die übrigen PDFs zum Download anzubieten, bei denen dies aktuell noch nicht möglich ist. Weitere Informationen hier.
Welcher Unterschied besteht bei den Preisen zwischen den Aboplänen?
Mit beiden Aboplänen erhältst du vollen Zugang zur Bibliothek und allen Funktionen von Perlego. Die einzigen Unterschiede bestehen im Preis und dem Abozeitraum: Mit dem Jahresabo sparst du auf 12 Monate gerechnet im Vergleich zum Monatsabo rund 30 %.
Was ist Perlego?
Wir sind ein Online-Abodienst für Lehrbücher, bei dem du für weniger als den Preis eines einzelnen Buches pro Monat Zugang zu einer ganzen Online-Bibliothek erhältst. Mit über 1 Million Büchern zu über 1.000 verschiedenen Themen haben wir bestimmt alles, was du brauchst! Weitere Informationen hier.
Unterstützt Perlego Text-zu-Sprache?
Achte auf das Symbol zum Vorlesen in deinem nächsten Buch, um zu sehen, ob du es dir auch anhören kannst. Bei diesem Tool wird dir Text laut vorgelesen, wobei der Text beim Vorlesen auch grafisch hervorgehoben wird. Du kannst das Vorlesen jederzeit anhalten, beschleunigen und verlangsamen. Weitere Informationen hier.
Ist Respiratory Medicine als Online-PDF/ePub verfügbar?
Ja, du hast Zugang zu Respiratory Medicine von Stephen J. Bourke, Graham P. Burns im PDF- und/oder ePub-Format sowie zu anderen beliebten Büchern aus Médecine & Médecine pulmonaire et thoracique. Aus unserem Katalog stehen dir über 1 Million Bücher zur Verfügung.
The anatomy and physiology of the respiratory system are designed in such a way as to bring air from the atmosphere and blood from the circulation into close proximity across the alveolar capillary membrane. This facilitates the exchange of oxygen and carbon dioxide between the blood and the outside world.
A brief revision of clinically relevant anatomy
Bronchial tree and alveoli
The trachea has cartilaginous horseshoe-shaped ‘rings’ supporting its anterior and lateral walls. The posterior wall is flaccid and bulges forward during coughing. This results in narrowing of the lumen, which increases the shearing force from the moving air on the mucus lying on the tracheal walls.
The trachea divides into the right and left main bronchi at the level of the sternal angle (angle of Louis). The left main bronchus is longer than the right and leaves the trachea at a more abrupt angle. The right main bronchus is more directly in line with the trachea, so that inhaled material tends to enter the right lung more readily than the left.
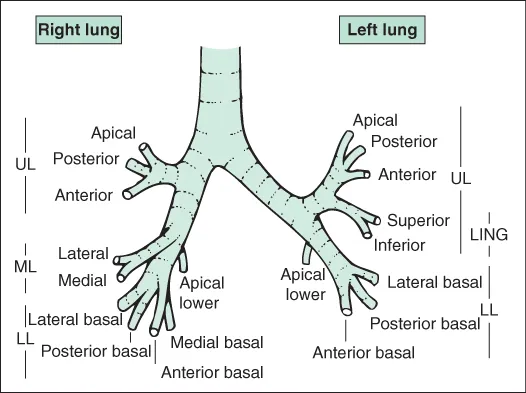
The main bronchi divide into lobar bronchi (upper, middle and lower on the right; upper and lower on the left) and then segmental bronchi, as shown in Fig. 1.1. The position of the lungs in relation to external landmarks is shown in Fig. 1.2. Bronchi are airways with cartilage in their walls, and there are about 10 divisions of bronchi beyond the tracheal bifurcation. Smaller airways without cartilage in their walls are referred to as bronchioles. Respiratory bronchioles are peripheral bronchioles with alveoli in their walls. Bronchioles immediately proximal to alveoli are known as terminal bronchioles. In the bronchi, smooth muscle is arranged in a spiral fashion internal to the cartilaginous plates. The muscle coat becomes more complete distally as the cartilaginous plates become more fragmentary.
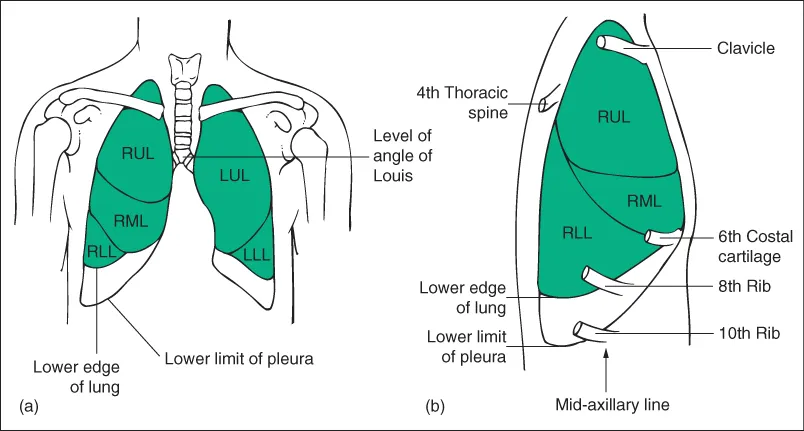
Figure 1.2 Surface anatomy. (a) Anterior view of the lungs. (b) Lateral view of the right side of the chest at resting end-expiratory position. LLL, left lower lobe; LUL, left upper lobe; RLL, right lower lobe; RML, right middle lobe; RUL, right upper lobe.
The epithelial lining is ciliated and includes goblet cells. The cilia beat with a whip-like action, and waves of contraction pass in an organised fashion from cell to cell so that material trapped in the sticky mucus layer above the cilia is moved upwards and out of the lung. This mucociliary escalator is an important part of the lung's defences. Larger bronchi also have acinar mucus-secreting glands in the submucosa, which are hypertrophied in chronic bronchitis.
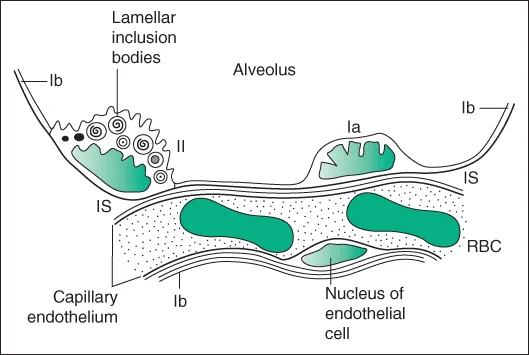
Alveoli are about 0.1–0.2 mm in diameter and are lined by a thin layer of cells, of which there are two types: type I pneumocytes have flattened processes that extend to cover most of the internal surface of the alveoli; type II pneumocytes are less numerous and contain lamellated structures, which are concerned with the production of surfactant (Fig. 1.3). There is a potential space between the alveolar cells and the capillary basement membrane, which is only apparent in disease states, when it may contain fluid, fibrous tissue or a cellular infiltrate.
Figure 1.3 Structure of the alveolar wall as revealed by electron microscopy. Ia, type I pneumocyte; Ib, flattened extension of type I pneumocyte covering most of the internal surface of the alveolus; II, type II pneumocyte with lamellar inclusion bodies, which are probably the site of surfactant formation; IS, interstitial space; RBC, red blood corpuscle. Pneumocytes and endothelial cells rest upon thin continuous basement membranes, which are not shown.
Lung perfusion
The lungs receive a blood supply from both the pulmonary and the systemic circulations.
The pulmonary artery arises from the right ventricle and divides into left and right pulmonary arteries, which further divide into branches accompanying the bronchial tree. The pulmonary capillary network in the alveolar walls is very dense and provides a very large surface area for gas exchange. The pulmonary venules drain laterally to the periphery of lung lobules and then pass centrally into the interlobular and intersegmental septa, ultimately joining together to form the four main pulmonary veins, which empty into the left atrium.
Several small bronchial arteries usually arise from the descending aorta and travel in the outer layers of the bronchi and bronchioles, supplying the tissues of the airways down to the level of the respiratory bronchiole. Most of the blood drains into radicles of the pulmonary vein, contributing a small amount of desaturated blood, which accounts for part of the ‘physiological shunt’ (blood passing through the lungs without being oxygenated) observed in normal individuals. The bronchial arteries may undergo hypertrophy when there is chronic pulmonary inflammation, and major haemoptysis in diseases such as bronchiectasis or aspergilloma usually arises from the bronchial rather than the pulmonary arteries and may be treated by therapeutic bronchial artery embolisation. The pulmonary circulation normally offers a much lower resistance and operates at a lower perfusion pressu...