Respiratory Medicine Lecture Notes covers everything from the basics of anatomy and physiology, through to the aetiology, epidemiology, symptoms and management of a full range of respiratory diseases, providing a comprehensive yet easy-to-read overview of all the essentials of respiratory medicine. Key features of this new, full-colouredition include: •Updated and expanded material on chest X-rays and radiology •Self-assessment exercises for each chapter •A range of clinical images and scans showing the key features of each disease •Fully supported by a companion website at www.lecturenoteseries.com/respiratory featuring figures, key points, web links, and interactive self-assessment questions Ideal for learning the basics of the respiratory system, starting a placement, or as a quick-reference revision guide, Respiratory Medicine Lecture Notes is an invaluable resource for medical students, respiratory nurses and junior doctors.
Foire aux questions
Comment puis-je résilier mon abonnement ?
Il vous suffit de vous rendre dans la section compte dans paramètres et de cliquer sur « Résilier l’abonnement ». C’est aussi simple que cela ! Une fois que vous aurez résilié votre abonnement, il restera actif pour le reste de la période pour laquelle vous avez payé. Découvrez-en plus ici.
Puis-je / comment puis-je télécharger des livres ?
Pour le moment, tous nos livres en format ePub adaptés aux mobiles peuvent être téléchargés via l’application. La plupart de nos PDF sont également disponibles en téléchargement et les autres seront téléchargeables très prochainement. Découvrez-en plus ici.
Quelle est la différence entre les formules tarifaires ?
Les deux abonnements vous donnent un accès complet à la bibliothèque et à toutes les fonctionnalités de Perlego. Les seules différences sont les tarifs ainsi que la période d’abonnement : avec l’abonnement annuel, vous économiserez environ 30 % par rapport à 12 mois d’abonnement mensuel.
Qu’est-ce que Perlego ?
Nous sommes un service d’abonnement à des ouvrages universitaires en ligne, où vous pouvez accéder à toute une bibliothèque pour un prix inférieur à celui d’un seul livre par mois. Avec plus d’un million de livres sur plus de 1 000 sujets, nous avons ce qu’il vous faut ! Découvrez-en plus ici.
Prenez-vous en charge la synthèse vocale ?
Recherchez le symbole Écouter sur votre prochain livre pour voir si vous pouvez l’écouter. L’outil Écouter lit le texte à haute voix pour vous, en surlignant le passage qui est en cours de lecture. Vous pouvez le mettre sur pause, l’accélérer ou le ralentir. Découvrez-en plus ici.
Est-ce que Respiratory Medicine est un PDF/ePUB en ligne ?
Oui, vous pouvez accéder à Respiratory Medicine par Stephen J. Bourke, Graham P. Burns en format PDF et/ou ePUB ainsi qu’à d’autres livres populaires dans Médecine et Médecine pulmonaire et thoracique. Nous disposons de plus d’un million d’ouvrages à découvrir dans notre catalogue.
The anatomy and physiology of the respiratory system are designed in such a way as to bring air from the atmosphere and blood from the circulation into close proximity across the alveolar capillary membrane. This facilitates the exchange of oxygen and carbon dioxide between the blood and the outside world.
A brief revision of clinically relevant anatomy
Bronchial tree and alveoli
The trachea has cartilaginous horseshoe-shaped ‘rings’ supporting its anterior and lateral walls. The posterior wall is flaccid and bulges forward during coughing. This results in narrowing of the lumen, which increases the shearing force from the moving air on the mucus lying on the tracheal walls.
The trachea divides into the right and left main bronchi at the level of the sternal angle (angle of Louis). The left main bronchus is longer than the right and leaves the trachea at a more abrupt angle. The right main bronchus is more directly in line with the trachea, so that inhaled material tends to enter the right lung more readily than the left.
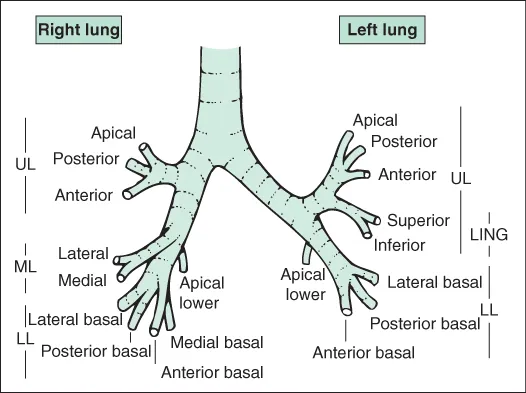
The main bronchi divide into lobar bronchi (upper, middle and lower on the right; upper and lower on the left) and then segmental bronchi, as shown in Fig. 1.1. The position of the lungs in relation to external landmarks is shown in Fig. 1.2. Bronchi are airways with cartilage in their walls, and there are about 10 divisions of bronchi beyond the tracheal bifurcation. Smaller airways without cartilage in their walls are referred to as bronchioles. Respiratory bronchioles are peripheral bronchioles with alveoli in their walls. Bronchioles immediately proximal to alveoli are known as terminal bronchioles. In the bronchi, smooth muscle is arranged in a spiral fashion internal to the cartilaginous plates. The muscle coat becomes more complete distally as the cartilaginous plates become more fragmentary.
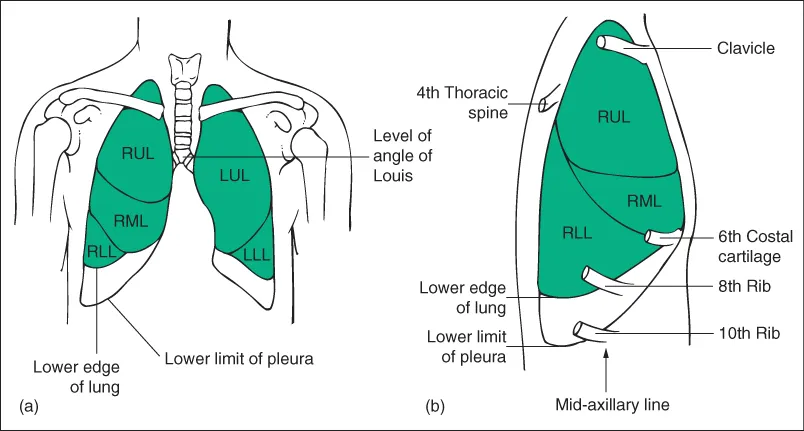
Figure 1.2 Surface anatomy. (a) Anterior view of the lungs. (b) Lateral view of the right side of the chest at resting end-expiratory position. LLL, left lower lobe; LUL, left upper lobe; RLL, right lower lobe; RML, right middle lobe; RUL, right upper lobe.
The epithelial lining is ciliated and includes goblet cells. The cilia beat with a whip-like action, and waves of contraction pass in an organised fashion from cell to cell so that material trapped in the sticky mucus layer above the cilia is moved upwards and out of the lung. This mucociliary escalator is an important part of the lung's defences. Larger bronchi also have acinar mucus-secreting glands in the submucosa, which are hypertrophied in chronic bronchitis.
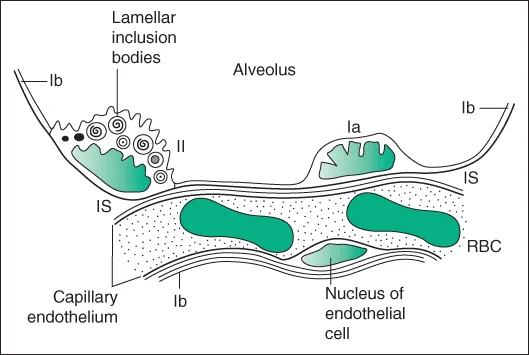
Alveoli are about 0.1–0.2 mm in diameter and are lined by a thin layer of cells, of which there are two types: type I pneumocytes have flattened processes that extend to cover most of the internal surface of the alveoli; type II pneumocytes are less numerous and contain lamellated structures, which are concerned with the production of surfactant (Fig. 1.3). There is a potential space between the alveolar cells and the capillary basement membrane, which is only apparent in disease states, when it may contain fluid, fibrous tissue or a cellular infiltrate.
Figure 1.3 Structure of the alveolar wall as revealed by electron microscopy. Ia, type I pneumocyte; Ib, flattened extension of type I pneumocyte covering most of the internal surface of the alveolus; II, type II pneumocyte with lamellar inclusion bodies, which are probably the site of surfactant formation; IS, interstitial space; RBC, red blood corpuscle. Pneumocytes and endothelial cells rest upon thin continuous basement membranes, which are not shown.
Lung perfusion
The lungs receive a blood supply from both the pulmonary and the systemic circulations.
The pulmonary artery arises from the right ventricle and divides into left and right pulmonary arteries, which further divide into branches accompanying the bronchial tree. The pulmonary capillary network in the alveolar walls is very dense and provides a very large surface area for gas exchange. The pulmonary venules drain laterally to the periphery of lung lobules and then pass centrally into the interlobular and intersegmental septa, ultimately joining together to form the four main pulmonary veins, which empty into the left atrium.
Several small bronchial arteries usually arise from the descending aorta and travel in the outer layers of the bronchi and bronchioles, supplying the tissues of the airways down to the level of the respiratory bronchiole. Most of the blood drains into radicles of the pulmonary vein, contributing a small amount of desaturated blood, which accounts for part of the ‘physiological shunt’ (blood passing through the lungs without being oxygenated) observed in normal individuals. The bronchial arteries may undergo hypertrophy when there is chronic pulmonary inflammation, and major haemoptysis in diseases such as bronchiectasis or aspergilloma usually arises from the bronchial rather than the pulmonary arteries and may be treated by therapeutic bronchial artery embolisation. The pulmonary circulation normally offers a much lower resistance and operates at a lower perfusion pressu...