![]()
Applied Technologies in Specific Clinical Situations
Technology in Sleep Pulmonary Disorders
Esquinas AM (ed): Applied Technologies in Pulmonary Medicine. Basel, Karger, 2011, pp 46–50
______________________
Thermal Infrared Imaging during Polysomnography: Has the Time Come to Unwire the ‘Wired’ Subjects?
Jayasimha N. Murthya · Ioannis Pavlidisb
aDivisions of Pulmonary, Critical Care and Sleep Medicine, University of Texas Health Science Center, and bDepartment of Computer Science, University of Houston, Houston, Tex., USA
______________________
Abbreviations
ATHEMOS | Automated thermal monitoring system |
BCI | Bayesian credible interval |
κ (kappa) | Chance-corrected agreement |
Pn | Nasal pressure – airflow monitoring device routinely used in polysomnography |
REM | Rapid eye movement |
RERA | Respiratory effort-related arousals |
SDB | Sleep disordered breathing – encompasses a wide variety of disorders characterized by breathing abnormalities during sleep such as obstructive sleep apnea, central sleep apnea, etc. |
TIRI | Thermal infrared imaging |
Untreated SDB is a very prevalent problem and can cause daytime sleepiness as well as have far-reaching socioeconomic and health-related consequences. A summary of statistics from three pooled studies estimated that 20% of adults with a body mass index between 25 and 28 kg/m2 have SDB based on an apnea-hypopnea index of >5 per hour [1]. Sleepiness is believed to have played a major role in causing disasters such as the Chernobyl and the Three Mile Island tragedies [2] and has been reported to be the most common cause of fatalities associated with motor vehicle accidents [3]. Untreated SDB is also associated with cardiovascular diseases [4].
Diagnosis of sleep apnea typically involves an overnight sleep study with simultaneous monitoring of airflow channels (Pn, oro-nasal thermistor), electrocardiogram, sleep staging by electroencephalography, electro oculography, and chin and leg electromyography in accordance with the Level 1 recommendations of the American Academy of Sleep Medicine [5]. However, conventional polysomnography has the potential to interfere with the ‘usual’ sleep pattern. A sizeable proportion of patients and normal volunteers who have never had a prior sleep study, experience the ‘first night effect’ characterized mainly by a decrease in sleep efficiency, prolongation of sleep-onset time, increase in REM sleep latency and a reduction in the total amount of REM sleep [6]. Additionally, it has been demonstrated that instrumentation during polysomnography affects body position during sleep [7] and thus impacts the diagnosis of SDB, the severity of which can increase during supine sleep. Moreover, bedside manipulation of sensors, in an effort to obtain high-quality data, may further disturb sleep and hinder our ability to obtain a true representation of the patient's usual sleep pattern. Thus, decreasing subject contact with monitoring equipment and testing in the ‘usual’ sleep environment may help counteract polysomnography's interference with sleep and SDB.
American Academy of Sleep Medicine recommends the use of thermistor as the airflow sensor for the diagnosis of apnea and Pn for the diagnosis of hypopnea as well as RERA [5]. While Pn can overestimate pathological events, especially when subjects change from nasal to predominantly oral breathing, the thermistor on the other hand lacks the sensitivity as compared to Pn, to detect subtle flow abnormalities such as hypopnea and RERAs. Non-contact airflow monitoring technology such as TIRI has the capability to monitor airflow during sleep without subject contact. This concept can be extended to include both laboratory-based and home-based sleep studies.
Description of TIRI
The principle of operation of TIRI is close to that of the oro-nasal thermistor in that both these methods sense thermal radiation. However, it is important to note the following differences between the thermistor and TIRI:
(1) TIRI can sense thermal information at a distance (contact-free), while the thermistor needs to be physically placed and tethered to patient's oro-nasal area, in the proximity of the thermal signal.
(2) TIRI acquires thermal information through natural radiation from the source as opposed to the thermistor which acquires thermal information by conduction when placed in the path of airflow. Theoretically, conduction is bidirectional and has an associated measurement error based on where and when the measurements are made. The accuracy also depends on the intensity as well as the magnitude of change in the thermal signal that is being measured. This error can be detrimental to the detection of subtle airflow abnormalities. TIRI, on the other hand, is an array (imaging sensor) and not just a point sensor-like thermistor. Therefore, it can be used to obtain a thermistor-like signal across time by averaging the thermal signal from all the points in the cross-sectional area of the visible nares, as well as provide thermal information over an extended two-dimensional surface. Analysis of signal as an evolving two-dimensional surface across increases the sensitivity of TIRI and may increase its ability to detect subtle airflow-related phenomena.
Thus, on theoretical grounds alone, one would expect TIRI to be considered a ‘virtual thermistor’ to perform at least as good as the oro-nasal thermistor [8]. Despite these inherent advantages of TIRI as compared to the thermistor, the following significant challenges had to be overcome to realize the translation of this technology for airflow monitoring:
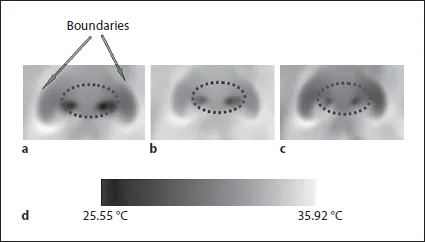
(1) Virtual probing: Since there is no physical probe involved in TIRI, a computational method is needed to segment the nostrils in the image, thus creating a ‘virtual’ probe, where the measurement can be performed. The difference in the temperature of inspired and expired air brings about a temporal variation in the thermal signature of the nostrils. This fluctuating thermal signal helps in the differentiation of the nostrils (or mouth, if the subject is mouth-breathing) from the rest of the facial tissue. The nostrils can thus be segmented from the face with the nasal cartilages forming ‘colder’ boundaries around the thermal signal (fig. 1).
(2) Tracking: Because there is no tethering and the subject is free to move, a computational method is needed to track changes in position, so that the virtual probe stays always in place and the accuracy of measurement is preserved. Functional imaging such as TIRI that maps randomly changing thermophysiological function in a non-restrained subject requires a collaborative network of particle filter trackers based on advanced statistics (coalitional tracking [9]) to compensate for subject movement.
Fig. 1. Temporal variance of nostril region in thermal imagery during breathing: (a) inspiration phase, (b) transition phase, (c) expiration phase, and (d) thermal color map. Note the cold boundaries (labeled ‘Boundaries’) of the nasal cartilages that allow the segmentation of nostrils from the rest of the facial tissue.
(3) Signal extraction: Assuming that virtual probing and tracking work well, they create the opportunity for a good measurement, but not the measurement in itself. Since there is no physical transducer that can produce an electronic signal in response to thermal signal, the signal has to be computationally generated. This has been achieved by continuous wavelet transformation on the normalized thermal signal under the assumption that the breathing component is the strongest part of the varying thermal signal.
Integration of TIRI with Polysomnography
The integrated hardware and software system we used in our preliminary study [10] is called ATHEMOS. The thermal signal acquired by the infrared camera and proce...