Clinical Approaches and Evidence of Success, Second Edition
Myron Nevins, Hom-Lay Wang
This is a test
This is a test
Partager le livre
544 pages
English
ePUB (adapté aux mobiles)
Disponible sur iOS et Android
eBook - ePub
Implant Therapy
Clinical Approaches and Evidence of Success, Second Edition
Myron Nevins, Hom-Lay Wang
Détails du livre
Aperçu du livre
Table des matières
Citations
À propos de ce livre
Since the publication of the first edition of this book 20 years ago, the landscape of implant dentistry has changed dramatically. Both the industry and patient demand have expanded exponentially, leaving the clinician with many decisions to make (and often as many questions to ask) regarding patient selection, surgical timing and techniques, implant types, and restorative approaches. This volume brings together the knowledge of the foremost leaders in implant dentistry, covering all aspects of the treatment process, from decision-making and treatment planning through imaging, surgical techniques, bone and soft tissue augmentation, multidisciplinary approaches, loading protocols, and finally strategies for preventing and treating complications and peri-implantitis as well as providing effective implant maintenance therapy. Filled with expert knowledge based on decades of research and clinical experience as well as abundant illustrations and clinical case presentations, this book is an indispensable resource for clinicians seeking to provide implant treatment at the highest standard of care.
Foire aux questions
Comment puis-je résilier mon abonnement ?
Il vous suffit de vous rendre dans la section compte dans paramètres et de cliquer sur « Résilier l’abonnement ». C’est aussi simple que cela ! Une fois que vous aurez résilié votre abonnement, il restera actif pour le reste de la période pour laquelle vous avez payé. Découvrez-en plus ici.
Puis-je / comment puis-je télécharger des livres ?
Pour le moment, tous nos livres en format ePub adaptés aux mobiles peuvent être téléchargés via l’application. La plupart de nos PDF sont également disponibles en téléchargement et les autres seront téléchargeables très prochainement. Découvrez-en plus ici.
Quelle est la différence entre les formules tarifaires ?
Les deux abonnements vous donnent un accès complet à la bibliothèque et à toutes les fonctionnalités de Perlego. Les seules différences sont les tarifs ainsi que la période d’abonnement : avec l’abonnement annuel, vous économiserez environ 30 % par rapport à 12 mois d’abonnement mensuel.
Qu’est-ce que Perlego ?
Nous sommes un service d’abonnement à des ouvrages universitaires en ligne, où vous pouvez accéder à toute une bibliothèque pour un prix inférieur à celui d’un seul livre par mois. Avec plus d’un million de livres sur plus de 1 000 sujets, nous avons ce qu’il vous faut ! Découvrez-en plus ici.
Prenez-vous en charge la synthèse vocale ?
Recherchez le symbole Écouter sur votre prochain livre pour voir si vous pouvez l’écouter. L’outil Écouter lit le texte à haute voix pour vous, en surlignant le passage qui est en cours de lecture. Vous pouvez le mettre sur pause, l’accélérer ou le ralentir. Découvrez-en plus ici.
Est-ce que Implant Therapy est un PDF/ePUB en ligne ?
Oui, vous pouvez accéder à Implant Therapy par Myron Nevins, Hom-Lay Wang en format PDF et/ou ePUB ainsi qu’à d’autres livres populaires dans Medicine et Dentistry. Nous disposons de plus d’un million d’ouvrages à découvrir dans notre catalogue.
A Clinical Decision: Save the Tooth or Place an Implant?
Treatment Planning Considerations
Treating Periodontally Compromised Teeth
The Endodontic Treatment Option
Treating Patients with Sound Periodontium and a Localized Problem
Periodontal Regeneration
Decision Making for Saving the Natural Dentition
Esthetic Considerations
The contemporary hallmark of a superior clinician is the ability to select therapies that are predictable and have long-lasting results. The question of whether to save a tooth or replace it with a dental implant is multifaceted, and the assessment requires a multidisciplinary approach to dental care. Giannobile and Lang have reported a trend over the past two decades toward a reduced emphasis in clinical practice to save compromised teeth.1 They suggest that clinicians should revisit the long and successful history of tooth maintenance, preserving the natural dentition without the rush to extract teeth and replace them with implants. Dental practitioners do a disservice to their patients and themselves when they fail to carefully weigh the advantages and disadvantages of such options in providing optimal oral health care delivery to patients.
TREATMENT PLANNING CONSIDERATIONS
Decisions made in treatment planning often determine the value of the result for the patient. Contemporary dentistry has benefited from the predictability of osseointegration,2–10 periodontal regeneration,11–29 successful endodontics,30 and prosthodontics, four compelling areas in which the clinician must be knowledgeable in order to make an informed decision regarding when to save the tooth or place an implant.
Nearly every patient asks the same questions during consultations. They are the following:
• How much discomfort will I endure?
• How many visits will be required?
• What will be the total treatment time?
• How will this affect my appearance?
• What is the financial commitment?
• What is the expected longevity of the treatment outcome?
There is minimal information available in evidence-based dentistry to assist in making many clinical decisions because of the number of variables that challenge the recruitment of populations for randomized controlled trials. As a result, when considering the prospect of replacing a maxillary first premolar with two roots, for example, clinicians eventually resort to their own clinical experience or case report publications. Considerations that must be made include the following:
• What is the distance from the apex of the tooth to an anatomical obstacle, and will it be necessary to augment the bone in the floor of the sinus (Figs 1-1a and 1-1b)?
Fig 1-1(a and b) It is impossible to have just one protocol for a maxillary first premolar. There is ample bone on the left side to accept an osseointegrated implant; however, if the maxillary first premolar were extracted on the right side it probably would be necessary to augment bone to receive an implant. (c and d) Cadaver material demonstrating the difference in bone levels between a patient with a healthy dentition and a patient who is severely compromised periodontally. The prime dictating factor relates to the length of the clinical root rather than the length of the anatomical root.
• What is the position of the roots of the tooth relative to each other and to the neighboring teeth?
• Is the tooth vital, and how intact is the tooth structure and the occlusal level of bone (Figs 1-1c and 1-1d)?
• What type of lip line and dental display does the patient have, and how will it affect the esthetics?
• Could the tooth be treated endodontically? (A 2009 report by Morris et al31 concluded that implants require more postoperative treatment than endodontically treated teeth, possibly a result of contemporary advancements. In addition, many endodontic complications, with the exception of fractured teeth, are resolvable.)
Implant patients fall into two general categories. The first includes individuals with teeth that are congenitally missing or damaged by trauma or root resorption (Fig 1-2). The second group has demonstrated susceptibility to inflammation that is evidenced by radiographic bone loss (Fig 1-3). Those in the first category require only tooth structure correction or replacement, whereas the second group presents the additional challenge of preventing or minimizing recurrent inflammation. The primary factor dictating decision making becomes the length of the clinical root, ie, that portion of the tooth that resides in the alveolar process (see Figs 1-1c and 1-1d). With a susceptible patient, it is advisable to eliminate the periodontal disease and provide a carefully constructed periodic maintenance program to reduce the risk of active inflammatory disease.32 The therapeutic result has to provide an environment that the patient and dental hygienist can maintain (see Fig 1-3).
Fig 1-2(a to c) A young woman with root resorption on the distal surface of the right central incisor. An esthetic dental display is very important to the patient. (d to f) The clinical and radiographic postoperative result after replacing the damaged tooth with an osseointegrated implant.
Fig 1-3(a) The patient presented for a periodontal regeneration procedure. The radiographic examination demonstrated intrabony defects that were not contained, therefore eliminating the possibility of periodontal regeneration. The two premolars were removed, the alveolar process underwent reconstruction, and two dental implants were placed. (b) A 3-year posttreatment radiograph illustrates significant recovery and no evidence of bone loss. (c) The bone-implant contact remains steady after 14 years. This demonstrates that patients susceptible to disease can accept osseointegrated implants successfully.
It is of paramount importance to recognize at the outset that it is possible, and in some instances preferable, to use the time-honored therapeutic approaches of conventional restorative dentistry. Although there is a lack of controlled studies in the discipline of periodontal prostheses, there is a paucity of significant randomized controlled human studies to support the clinical application of many periodontal and prosthetic approaches. There is, however, overwhelmingly positive clinical evidence gathered through the observation of treated patients to be considered. Periodontally compromised patients with mobile, drifting, or missing teeth have been successfully rehabilitated with or without implants (Figs 1-3 to 1-5). Such patients require a treatment plan that provides predictability over an extended time frame.
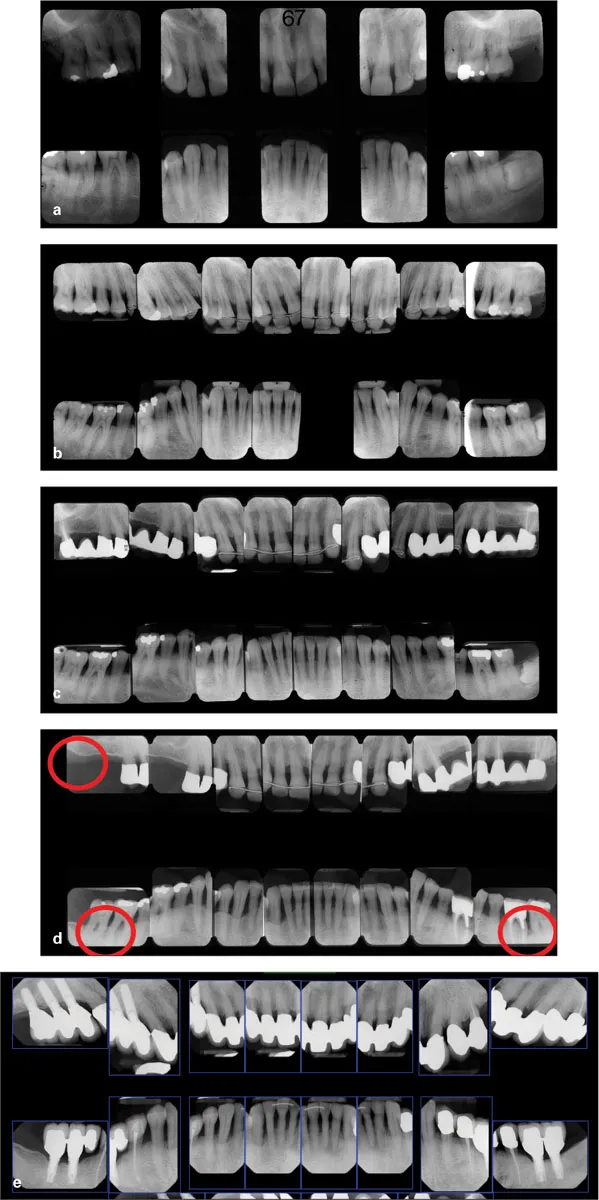
Fig 1-4(a) The patient presented with generalized advanced periodontitis. (b) A radiographic survey 1 year after the placement of many dental implants. Red circles indicate post and core risk. (c and d) Radiographic and clinical observation after 7 years. The maxillary left canine suffered a vertical root fracture and was replaced by a third 18-mm implant. The molar was removed and replaced with a cantilever. (e and f) Clinical presentation after 17 years. (g) A radiographic survey after 25 years. Once again, this demonstrates that people susceptible to periodontal disease can be treated successfully with osseointegrated implants.
Fig 1-5(a and b) Before and after radiographic surveys of a patient clearly susceptible to inflammatory periodontal disease. (c) A 13-year radiographic survey demonstrating the replacement of the maxillary first molars with fixed restorative d...