Medical Microbiology Illustrated
S. H. Gillespie
- 296 pages
- English
- ePUB (adapté aux mobiles)
- Disponible sur iOS et Android
Medical Microbiology Illustrated
S. H. Gillespie
À propos de ce livre
Medical Microbiology Illustrated presents a detailed description of epidemiology, and the biology of micro-organisms. It discusses the pathogenicity and virulence of microbial agents. It addresses the intrinsic susceptibility or immunity to antimicrobial agents. Some of the topics covered in the book are the types of gram-positive cocci; diverse group of aerobic gram-positive bacilli; classification and clinical importance of erysipelothrix rhusiopathiae; pathogenesis of mycobacterial infection; classification of parasitic infections which manifest with fever; collection of blood for culture and control of substances hazardous to health. The classification and clinical importance of neisseriaceae is fully covered. The definition and pathogenicity of haemophilus are discussed in detail. The text describes in depth the classification and clinical importance of spiral bacteria. The isolation and identification of fungi are completely presented. A chapter is devoted to the laboratory and serological diagnosis of systemic fungal infections. The book can provide useful information to microbiologists, physicians, laboratory scientists, students, and researchers.
Foire aux questions
Informations
Introduction to clinical microbiology
Publisher Summary
Introduction
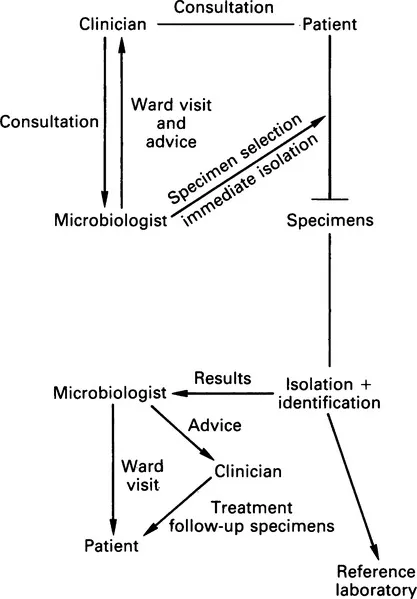
The process of microbiological diagnosis
Specimens
Specimen types
Specimen choice
Containers