A comprehensive review of the impact of dietary nutraceuticals on platelet function and its relationship to cardiovascular disease
Nutraceuticals and Human Blood Platelet Function offers a summary of the most current evidence on the effects of anti-platelet factors isolated mainly from food and natural sources, their structure function relationship, bioavailability, mechanisms of actions, and also information on human trials data. The author—a noted expert in the field— explores platelet function and their roles in development of CVD, functional foods and bioactive compounds in CVD risk factors. The author highlights platelets, their mechanisms of actions, data from epidemiological studies, structure-function relationship clinical trial data, ex vivo and in vitro data.
This important resource will focus primarily on human studies and emphasize functional and physiological implications of the nutritional impact on platelet function and CVD that could be an important approach to highlight the concept of preventive CVD nutrition. An authoritative text, Nutraceuticals and Human Blood Platelet Function:
Offers a unique resource that connects nutrition with platelet function and its impact on cardiovascular disease
Contains an evidenced-based approach, including data from human and animal clinical studies
Reveals the impact of bioactive compounds and their effect on platelets
Presents a text that is authored by an expert with vast experience in the field of nutrition and platelet function
Written for professionals, academics, researchers, and students associated in the area of nutrition, Nutraceuticals and Human Blood Platelet Function offers a review of the most current research on the effects of platelet function and their roles in development of CVD, functional foods and bioactive compounds in CVD risk factors.
Foire aux questions
Comment puis-je résilier mon abonnement ?
Il vous suffit de vous rendre dans la section compte dans paramètres et de cliquer sur « Résilier l’abonnement ». C’est aussi simple que cela ! Une fois que vous aurez résilié votre abonnement, il restera actif pour le reste de la période pour laquelle vous avez payé. Découvrez-en plus ici.
Puis-je / comment puis-je télécharger des livres ?
Pour le moment, tous nos livres en format ePub adaptés aux mobiles peuvent être téléchargés via l’application. La plupart de nos PDF sont également disponibles en téléchargement et les autres seront téléchargeables très prochainement. Découvrez-en plus ici.
Quelle est la différence entre les formules tarifaires ?
Les deux abonnements vous donnent un accès complet à la bibliothèque et à toutes les fonctionnalités de Perlego. Les seules différences sont les tarifs ainsi que la période d’abonnement : avec l’abonnement annuel, vous économiserez environ 30 % par rapport à 12 mois d’abonnement mensuel.
Qu’est-ce que Perlego ?
Nous sommes un service d’abonnement à des ouvrages universitaires en ligne, où vous pouvez accéder à toute une bibliothèque pour un prix inférieur à celui d’un seul livre par mois. Avec plus d’un million de livres sur plus de 1 000 sujets, nous avons ce qu’il vous faut ! Découvrez-en plus ici.
Prenez-vous en charge la synthèse vocale ?
Recherchez le symbole Écouter sur votre prochain livre pour voir si vous pouvez l’écouter. L’outil Écouter lit le texte à haute voix pour vous, en surlignant le passage qui est en cours de lecture. Vous pouvez le mettre sur pause, l’accélérer ou le ralentir. Découvrez-en plus ici.
Est-ce que Nutraceuticals and Human Blood Platelet Function est un PDF/ePUB en ligne ?
Oui, vous pouvez accéder à Nutraceuticals and Human Blood Platelet Function par Asim K. Duttaroy en format PDF et/ou ePUB ainsi qu’à d’autres livres populaires dans Technology & Engineering et Food Science. Nous disposons de plus d’un million d’ouvrages à découvrir dans notre catalogue.
Human blood platelets are non‐nucleated cells, produced in bone marrow from megakaryocytes [1]. Although very dynamic, blood platelets (around 2μm in diameter) usually prefer to remain in inactive state in circulation, and get activated only when a blood vessel is damaged [1, 2]. The human body produces and removes 1011 platelets daily to maintain a normal steady state platelet count. Platelet production must be regulated to avoid spontaneous bleeding or arterial occlusion and organ damage.
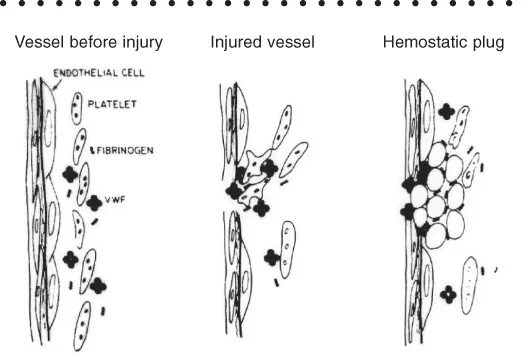
The primary physiological role of platelets is to sense the damaged vessel endothelium and rapidly accumulate at the damaged site of the vessel, where they initiate blood coagulation process to stop the bleeding (Figure 1.1).
Figure 1.1 The role of platelets in the blood vessel.
Circulating inactive platelets are biconvex but, upon activation, they become irregular and sticky, extending pseudopods and adhering to neighboring structures or aggregating with one another. The rapid interactions between activated platelets, their secreted components, or thrombin and endothelium at sites of damaged vessels, ensure the intravascular growth of the stable haemostatic plug [2].
Two different pathways mediate vascular homeostasis and thrombosis depending on vascular damage or vessel structure [1]. One is the intrinsic pathway mediated by collagen, while the other is the extrinsic pathway mediated by tissue factor(TF)‐factor‐VII complex. During normal hemostasis, damage to the endothelium may occur, and collagen from the sub‐endothelial space is exposed.
Platelets, through their glycoproteins (GP) GPVI and GPIb/V/IX, interact with collagen and von Willebrand factor (vWF). Collagen exposure leads to platelet adhesion and formation of a platelet monolayer on the damaged surface of the vessel. Platelets form a three‐dimensional structure by aggregating through their activated GPIIb/IIIa complexes, the fibrinogen receptors. Activated platelets aggregate with other circulating platelets by secreting platelet aggregatory/activating agents, such as thrombin, ADP, collagen, TxA2, and adrenaline. All these lead to the expression of fibrinogen receptors (GPIIb/IIIa complexes) [2].
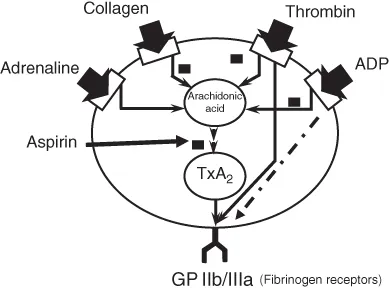
Figure 1.2 shows the expression of platelet membrane surface GPIIb/IIIa complexes induced by different aggregating agents through TxA2 formation from ARA, liberated from membrane phospholipids. The tissue damage or plaque rupture leads to the release of TF from smooth muscle, adventitial cells, and pericytes. TF, with the help of activated factor VII(VIIa), mediates the conversion of pro‐thrombin to thrombin, fibrin generation, and thus initiates the clotting cascade [1]. Activated platelets also accelerate the action of prothrombinase complex to produce thrombin from prothrombin.
Figure 1.2 Expression of fibrinogen receptors. Fibrinogen receptors (GPIIb/IIIa complex) on the platelet surface represents the final common pathway, whereby platelet stimulation by various agonists leads to fibrinogen binding, platelet aggregation, and thrombus formation. Aspirin can inhibit collagen, adrenaline and, to some extent, ADP‐induced expression of fibrinogen expression, but not the thrombin‐induced expression of GPIIb/IIIa complex on platelet surface.
Apart from hemostasis, platelets are involved in several processes in the cardiovascular system, such as atherosclerosis process, immune system, inflammation, and cardiac events [3–5]. Thus, human blood platelets play many pivotal roles in the pathophysiology of different diseases, from CVDs to tumor metastasis [6].
Upon activation, platelets secrete more than 300 components from their intracellular stores. Platelet dense granule components, such as ADP and polyphosphates, and Ca2+, contribute to blood coagulation and platelet aggregation. α‐Granules secrete multiple cytokines, mitogens, and other components that contribute to the CVD processes. Anucleated platelets have stable mRNA transcripts with a long life, and use a variety of mechanisms to translate these mRNAs into proteins [7].
There are two important key regulators of translation processes such as ELF‐4e and ELF‐2a that are used by platelets. Platelets synthesize several proteins, such as integrins, αIIbβ3, TF, plasminogen activator inhibitor‐1 (PAI‐1), cyclooxygenase (COX), Factor XI, protein C inhibitor CCL5/ RANTES, and IL‐1B [7]. mRNA translation is also regulated by miRNA in human platelets. In fact, the possibility of using miRNAs as biomarkers of atherosclerosis and cardiac episodes has been suggested. In platelets constitutively are synthesized proteins such as actin, PDGF, glycoproteins GPIIb/IIIa, and P‐selectin [7].
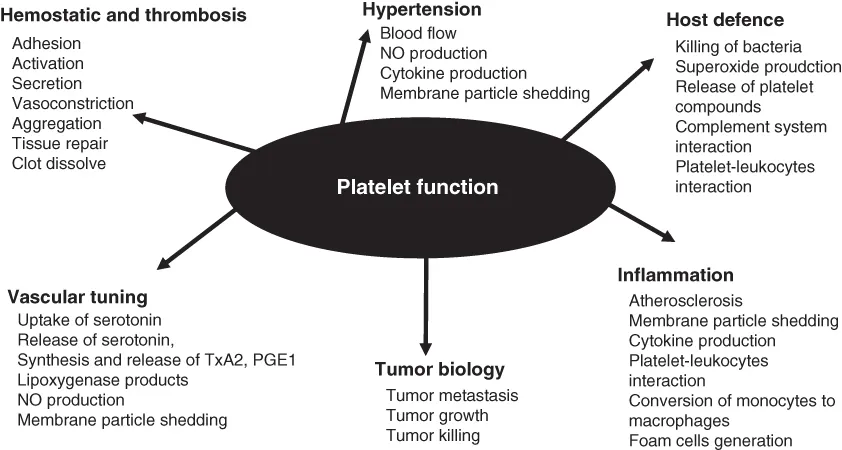
Platelet hyperactivity, as occurs in obesity, smoking, sedentary life styles, and diabetes, insulin resistance is associated with secretion of different components, along with the shedding of membrane particles that play important roles in the development of CVD risk, especially in the development of atherosclerosis, blood flow, inflammation, and hypertension (Figure 1.3).
Figure 1.3 The multiple roles of platelets in different diseases.
Continued research has revealed that platelet micro‐particles have numerous functions. In addition to atherosclerosis, they are involved in thrombus and foam cells formation, and inflammation. Platelet membrane proteins GPIbα, GPV, GPVI, amyloid βA4, TLT‐1 (TREM‐like transcript‐1), P‐selectin (CD40L), amyloid‐like protein 2 and semaphorin 4D are the most abundantly shed platelet proteins.
In this chapter, current understanding of human blood platelets and their roles in the development of CVD is discussed.
1.2 Human Blood Platelets: Structure and Function
Platelets have granular cytoplasm with no nucleus, and their diameter averages 2.5 µm, with a subpopulation of larger diameter 4–5 µm. Individual platelets, however, vary in terms of volume, density and reactivity towards agonists. The normal blood platelet count is in the range of 150–400 × 109/L. Under normal conditions, platelets circulate in the bloodstream for 8–10 days. Under conditions of hemostatic requirements, platelets move from the spleen to the peripheral blood circulation (70% of total platelets).
The normal peripheral blood platelet count is 150–400,000/μL [8]. This count represents only two‐thirds of available platelets, because the spleen retains the rest of the platelets. Megakaryocytes develop in the bone marrow from hematopoietic stem cells [9]. The megakaryocyte unde...