- 192 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
This excellent book is long overdue. It will be of benefit to anyone with an interest in general practitioner education, and anyone considering applying for the post of course organiser should read the opening chapters to prepare them for interview. This is a thoughtful book, written in a clear and witty style and it deserves a wide readership. It provides an educational framework on which general practitioner teaching can be based.' British Journal of General Practice This book is excellent because it deals not only with the nuts and bolts' of being a course organizer, but also addresses the difficulties, frustrations and emotions involved in a witty and entertaining manner. Anyone with an interest in postgraduate medical education, at any level, would benefit from reading this book.' Update Paddy McEvoy's book has rapidly and deservedly established itself as invaluable to anyone responsible for any form of postgraduate medical education.' Education for General Practice 'As well as updating and revising the book throughout. Paddy McEvoy has managed to include sections about the wider context of training without making the book overly long or losing any of the delightful flavour of the first edition. I have no doubt that you will find it both useful and enjoyable.''
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineChapter 1
The policy context for substance misuse services in primary care
Duncan Williams
What’s happening to primary care?
On 1 April 2004 GPs signed up to a new national contract to provide primary care within the National Health Service (NHS) via the organisation of practice teams rather than the historical individualised and hierarchical mechanisms of personal medical lists.1 The new contract challenges the team to provide a quality health agenda and offers incentives and opportunities to develop innovative approaches to care. This chapter discusses ideas relevant to current primary care which can be adapted within your practice to facilitate your professional development in the field of substance misuse. This will enable us to maximise more quality options for our patients. You are strongly recommended to follow the learning approach found in the Royal College of General Practitioners (RCGP) certificate in Substance Misuse course and develop your own portfolio of experience, critical reading skills and reflective learning technique.
The following is a checklist of primary care principles.
- It exists in the real world.
- It is local.
- It is accessible and realistic.
- It is long term.
- It takes a ‘full-length feature film look’ at people’s lives in the context of their health.
- ‘Snapshots’, although useful, belong more in rescue medicine than planned holistic management of chronic health problems which is the strength of primary care.
- It needs to be patient centred but often it isn’t.
Stop here
- In your practice, are you confident you apply these principles to your patients with substance misuse problems?
- Could you pick up one of your existing cases and quickly establish:
- – the initial treatment goals
- – the motivational factors for behavioural change
- – the actions to be taken if review reveals unmet need or variance from direction of progress?
Contracts in context
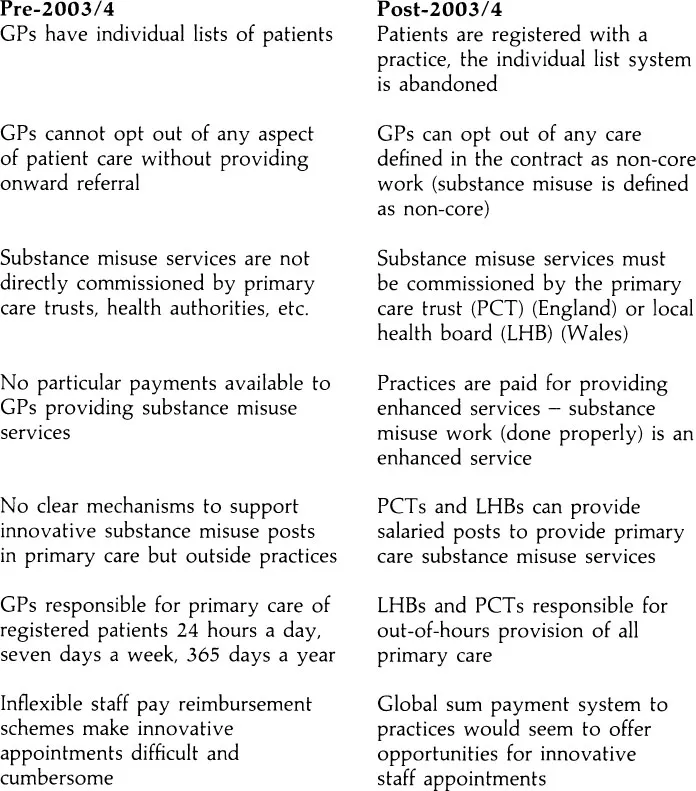
Box 1.1 Changes in substance misuse work after the new GMS contract
The new General Medical Services (GMS) Contract (2003) is the mechanism by which the government contracts for primary care services from general medical practitioners, on behalf of the nation. This provides the framework for organisation of all primary care, both directly within practices and indirectly, including non-directly employed staff included in their practical working arrangements.
Historically since the inception of the NHS, general practitioners (GPs) and their employed staff have contracted with the government of the day to provide GMS via a national contract. Fundholding in the 1990s gave budgets directly to practices to manage the interface between primary and secondary care for non-acute healthcare, although GPs continued to be paid contractually via the GMS contract. Fundholding was abolished in 1997, during the first term of the Labour government. A new contract was offered to practices who wished to have a variance on the nationally agreed GMS contract and a number of pilot schemes were established in 1998, these personal medical services (PMS) contracts now form 40% of the contractual arrangements between GPs and the NHS.2 Personal medical services contracts allow practices in areas of particular need to be paid for organising care along different lines to the standard GMS contract. This enables the practices to take into account any particular local needs, e.g. practices offering services to the homeless, the elderly, nurse-led services, etc.
The new contract introduced in April 2004 relates to the GMS contract. Pilot PMS schemes ended in March 2004 and PMS is now a permanent alternative to new GMS. Personal medical services contracts have not changed as a result of these new contracts but there are variations including ‘PCT-MS’, ‘PMS plus’ and ‘Specialist PMS’. These innovative schemes will allow providers to specialise in areas of care at a primary level (i.e. accessible and long term) without the provider being expected to deliver the totality of essential primary care. The important changes of the new GMS contract in the context of substance misuse work compared to the previous one are shown in Box 1.1.
Box 1.2 illustrates the changes to patient handling that occurred as a result of the new GMS contract.
Box 1.2 Example of change in patient handling
On 31 March 2004, JB attended his GP surgery looking for help with his heroin addiction. The receptionist said ‘Our list is full. We don’t want your sort here. Come back tomorrow’.
On 1 April 2004, JB went to his primary care practice and read the notice about the new nurse-led substance misuse assessment and prescribing service. He asked the receptionist if he could enrol and was given a cup of tea and asked to return next week.
Stop here
- Did you attend all those practice development meetings last year?
- Did you plan for this enormous shift in attitude?
The access agenda
Substance misuse patients without access to services die on waiting lists — an untenable disgrace!3
Governments and NHS policy makers of all political hues trumpet rapid access to services as a key target for the NHS.4 (Indeed few professionals would disagree with this aspiration.) However the increase in funding and staff needed to deliver rapid access has not been forthcoming, e.g. 24-hour waiting times to be seen by a GP. Much recent effort has been focused on improving systems of access and flexibility.
Many practices have undergone extensive restructuring and retraining programmes with the express purpose of providing rapid access for patients to the appropriate team member best able to meet their needs.5 The GP is perhaps best placed to provide investigative and diagnostic skills. The practice nurse could lead on disease management skills, treatment compliance and patient motivating skills, and disease or chronic condition monitoring. The health visitor could lead on primary prevention and child and adolescent mental health.
- What is your practice doing about access?
- Are you involved in the processes of change? (If not why not?)
- Do you have untapped potential?
- Is your team aware of it? Do you need to speak with the practice manager today?
Innovation and service development
Primary care is the melting pot for innovation and organisational experimentation. It is made up of individuals in small teams, with regular contact and interaction between members, many of whom have intimate and long-term knowledge of the families and circumstances of our patients. Team meetings are a feature of good primary care arrangements and these lend themselves to discussion and planned change, critical case analysis, near misses and hot topic discussions. All these are familiar concepts to the committed primary care enthusiast.
Box 1.3 illustrates a system failure.
Box 1.3
JB attended his GP two years ago to ask for treatment for his heroin addiction and was told he’d be referred to the local hospital trust – on 1 April he is still on the waiting list.
The development of local services for substance misusers depends upon individuals prepared to challenge the status quo in their own practice environment and to embrace change as an opportunity to provide something new that currentl...
Table of contents
- Cover
- Title Page
- Copyright Page
- Contents
- Foreword
- Preface
- About the editor
- List of contributors
- List of abbreviations
- Chapter 1 The policy context for substance misuse services in primary care
- Chapter 2 Practical guide for the addiction nurse in shared care
- Chapter 3 Users and practitioners: an equal partnership
- Chapter 4 The role of the practice nurse in substance misuse treatments
- Chapter 5 Primary care nursing and alcohol: a new way forward?
- Chapter 6 The role of the midwife working with a pregnant drug user
- Chapter 7 The role of the health visitor in relation to child protection and substance misuse
- Chapter 8 Treatment and its effectiveness in relapse prevention associated with crack cocaine
- Chapter 9 The role of the practice counsellor in substance misuse treatments
- Chapter 10 Special issues for effective treatment of homeless drug users
- Chapter 11 The complex world of dual diagnosis, nursing and primary care
- Chapter 12 Future directions and partnerships: the way forward for nursing
- Appendix 1 Sample methadone prescribing protocol
- Appendix 2 Sample Subutex prescribing protocol
- Appendix 3 Luther Street policy for the management of contacts with the addictions team
- Appendix 4 DANOS competencies for addiction nurses
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Substance Misuse in Primary Care by Rosie Winyard in PDF and/or ePUB format, as well as other popular books in Medicine & Medical Theory, Practice & Reference. We have over 1.5 million books available in our catalogue for you to explore.