
eBook - ePub
Atlas of Diagnostic Endoscopy, 3E
Mohammad Ibrarullah
This is a test
Buch teilen
- 186 Seiten
- English
- ePUB (handyfreundlich)
- Über iOS und Android verfügbar
eBook - ePub
Atlas of Diagnostic Endoscopy, 3E
Mohammad Ibrarullah
Angaben zum Buch
Buchvorschau
Inhaltsverzeichnis
Quellenangaben
Über dieses Buch
This book is a compilation of endoscopic images of the upper gastrointestinal tract. The 3rd edition is enriched with high-resolution digital images highlighting the classification and staging of endoscopically relevant diseases. Serial documentation of diseases and procedures like corrosive injury, variceal obliteration, peptic ulcer etc. provides a complete, informative and interesting perspective. Rare conditions like Dieulafoy's disease and Gastric antral vascular ectasia (GAVE) have been extensively discussed along with common diseases of the GI tract. This book outlines the technique and interpretation of endoscopic images proving to be a helpful guide to endoscopy practitioners.
Key Features
-
- Explores various GI tract diseases through coloured, high resolution clinical photographs.
-
- Serves as a useful reckoner for trainee endoscopists and practitioners pursuing gastroenterology or gastrointestinal endoscopy.
-
- The text is updated with tables, flowcharts, classifications and international treatment guidelines.
Häufig gestellte Fragen
Wie kann ich mein Abo kündigen?
Gehe einfach zum Kontobereich in den Einstellungen und klicke auf „Abo kündigen“ – ganz einfach. Nachdem du gekündigt hast, bleibt deine Mitgliedschaft für den verbleibenden Abozeitraum, den du bereits bezahlt hast, aktiv. Mehr Informationen hier.
(Wie) Kann ich Bücher herunterladen?
Derzeit stehen all unsere auf Mobilgeräte reagierenden ePub-Bücher zum Download über die App zur Verfügung. Die meisten unserer PDFs stehen ebenfalls zum Download bereit; wir arbeiten daran, auch die übrigen PDFs zum Download anzubieten, bei denen dies aktuell noch nicht möglich ist. Weitere Informationen hier.
Welcher Unterschied besteht bei den Preisen zwischen den Aboplänen?
Mit beiden Aboplänen erhältst du vollen Zugang zur Bibliothek und allen Funktionen von Perlego. Die einzigen Unterschiede bestehen im Preis und dem Abozeitraum: Mit dem Jahresabo sparst du auf 12 Monate gerechnet im Vergleich zum Monatsabo rund 30 %.
Was ist Perlego?
Wir sind ein Online-Abodienst für Lehrbücher, bei dem du für weniger als den Preis eines einzelnen Buches pro Monat Zugang zu einer ganzen Online-Bibliothek erhältst. Mit über 1 Million Büchern zu über 1.000 verschiedenen Themen haben wir bestimmt alles, was du brauchst! Weitere Informationen hier.
Unterstützt Perlego Text-zu-Sprache?
Achte auf das Symbol zum Vorlesen in deinem nächsten Buch, um zu sehen, ob du es dir auch anhören kannst. Bei diesem Tool wird dir Text laut vorgelesen, wobei der Text beim Vorlesen auch grafisch hervorgehoben wird. Du kannst das Vorlesen jederzeit anhalten, beschleunigen und verlangsamen. Weitere Informationen hier.
Ist Atlas of Diagnostic Endoscopy, 3E als Online-PDF/ePub verfügbar?
Ja, du hast Zugang zu Atlas of Diagnostic Endoscopy, 3E von Mohammad Ibrarullah im PDF- und/oder ePub-Format sowie zu anderen beliebten Büchern aus Medicina & Teoría, práctica y referencia médicas. Aus unserem Katalog stehen dir über 1 Million Bücher zur Verfügung.
Information
1
Techniques of UGI endoscopy and normal anatomy
Preparation for endoscopy
Informed consent and counseling: The patient should be clearly informed about the procedure and the likely discomfort he may experience. It should be explained that his cooperation will make the procedure easier and quicker.
Overnight fasting: Routine endoscopy is usually performed in the morning hours after overnight fasting. Coating agents like antacids or colored medications should be clearly withheld. In case of obstructed stomach, prior nasogastric intubation and lavage should be performed to clear the gastric residue.
Sedation and anesthesia: For routine UGI endoscopy, we use only topical pharyngeal anesthetics such as lignocaine viscous or spray. Sedation, in the form of intravenous Midazolam, is occasionally used in children. For therapeutic endoscopy, such as foreign body removal, stent placement etc., it is our practice to use intravenous propofol anesthesia with or without endotracheal intubation.
Endotracheal intubation and monitoring: Endoscopy in a comatose or irritable patient is fraught with the risk of aspiration, hypoxia and “bite” damage to the endoscope. It is our practice to use prior endotracheal intubation and also monitor the vital parameters during the procedure.
Instrument check: Prior to endoscopy, it is good practice to check the instrument, including the light source, suction channel, airflow and display panel for any malfunction.
Position of the patient: Diagnostic endoscopy is always performed in the left lateral position. Occasionally, in a patient with upper GI bleeding, it may be necessary to examine the patient in the right lateral position. This is to displace the fundal blood pool that may obscure the bleeding lesion.
Antibiotic prophylaxis: Antibiotic prophylaxis is not indicated for diagnostic endoscopy. Current recommendations by the American Society for Gastrointestinal Endoscopy (ASGE) exclude even conditions such as valvular heart disease, prosthetic valves, synthetic vascular graft and prosthetic joints from the ambit of antibiotic prophylaxis. The few indications for antibiotic prophylaxis are therapeutic endoscopy for cirrhosis with acute variceal bleeding, cyst drainage and in patients with established GI tract infection who have the above listed cardiovascular status.
The mouth guard is held between the teeth. It is further supported by the index and middle finger of the endoscopy assistant. Alternatively, an elastic band attached to the mouth guard can be used to keep it steady.
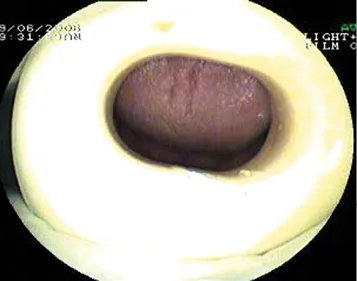
Figure 1.1 The mouth guard.
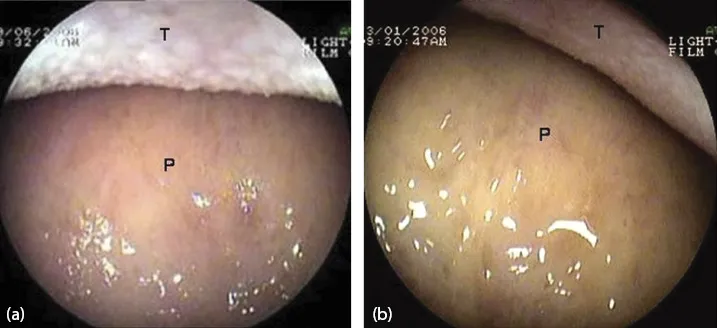
Figure 1.2 View as the endoscope enters the oral cavity. (a, b) Dorsum of the tongue (T) and hard palate (P).
The tip of the endoscope is slightly bent to fit the contour of the tongue. It is gently advanced over the base of the tongue towards the pharynx.
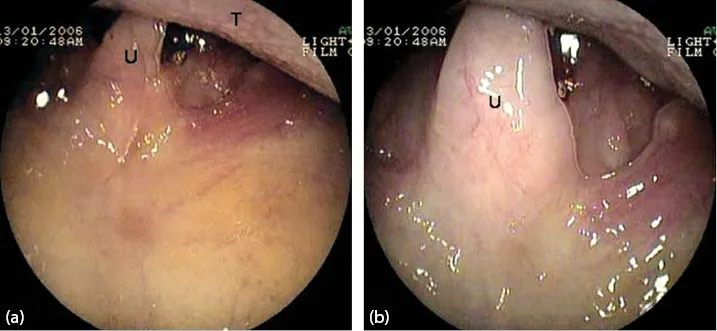
Figure 1.3 (a, b) Uvula (U) and the base of the tongue (T).
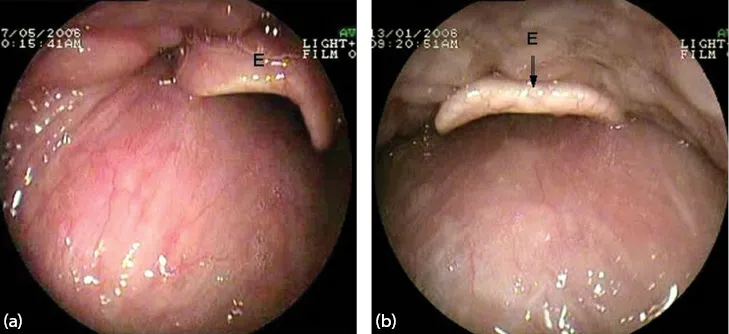
Figure 1.4 (a, b) Epiglottis (E).
The epiglottis (E) is seen as the pharynx is entered.
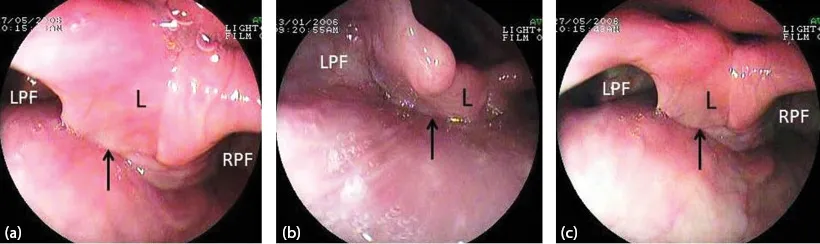
Figure 1.5 (a–c) The laryngo-pharynx. Larynx (L) and both pyriform fossae (RPF, LPF). The arrow points to the esophageal inlet.
As the scope passes below the epiglottis, the larynx and both pyrifo...