
eBook - ePub
OCT Angiography in Retinal and Macular Diseases
F. Bandello, E. H. Souied, G. Querques
This is a test
Buch teilen
- 184 Seiten
- English
- ePUB (handyfreundlich)
- Über iOS und Android verfügbar
eBook - ePub
OCT Angiography in Retinal and Macular Diseases
F. Bandello, E. H. Souied, G. Querques
Angaben zum Buch
Buchvorschau
Inhaltsverzeichnis
Quellenangaben
Über dieses Buch
In only a short period of time, the innovative procedure of OCT angiography has become an essential macula imaging technique. Now that it is routinely used in clinical practice, the investigation of retinal and choroidal circulation is non-invasive, which significantly changes the professional's approach to patients. In this volume, retina specialists and renowned experts share their experience with OCT angiography. They have included numerous color images and presented current ideas to form a base for further research and discussion. This book provides retina specialists, ophthalmologists, and researchers with a first glance at original research and clinical reports on this new methodology.
Häufig gestellte Fragen
Wie kann ich mein Abo kündigen?
Gehe einfach zum Kontobereich in den Einstellungen und klicke auf „Abo kündigen“ – ganz einfach. Nachdem du gekündigt hast, bleibt deine Mitgliedschaft für den verbleibenden Abozeitraum, den du bereits bezahlt hast, aktiv. Mehr Informationen hier.
(Wie) Kann ich Bücher herunterladen?
Derzeit stehen all unsere auf Mobilgeräte reagierenden ePub-Bücher zum Download über die App zur Verfügung. Die meisten unserer PDFs stehen ebenfalls zum Download bereit; wir arbeiten daran, auch die übrigen PDFs zum Download anzubieten, bei denen dies aktuell noch nicht möglich ist. Weitere Informationen hier.
Welcher Unterschied besteht bei den Preisen zwischen den Aboplänen?
Mit beiden Aboplänen erhältst du vollen Zugang zur Bibliothek und allen Funktionen von Perlego. Die einzigen Unterschiede bestehen im Preis und dem Abozeitraum: Mit dem Jahresabo sparst du auf 12 Monate gerechnet im Vergleich zum Monatsabo rund 30 %.
Was ist Perlego?
Wir sind ein Online-Abodienst für Lehrbücher, bei dem du für weniger als den Preis eines einzelnen Buches pro Monat Zugang zu einer ganzen Online-Bibliothek erhältst. Mit über 1 Million Büchern zu über 1.000 verschiedenen Themen haben wir bestimmt alles, was du brauchst! Weitere Informationen hier.
Unterstützt Perlego Text-zu-Sprache?
Achte auf das Symbol zum Vorlesen in deinem nächsten Buch, um zu sehen, ob du es dir auch anhören kannst. Bei diesem Tool wird dir Text laut vorgelesen, wobei der Text beim Vorlesen auch grafisch hervorgehoben wird. Du kannst das Vorlesen jederzeit anhalten, beschleunigen und verlangsamen. Weitere Informationen hier.
Ist OCT Angiography in Retinal and Macular Diseases als Online-PDF/ePub verfügbar?
Ja, du hast Zugang zu OCT Angiography in Retinal and Macular Diseases von F. Bandello, E. H. Souied, G. Querques im PDF- und/oder ePub-Format sowie zu anderen beliebten Büchern aus Medizin & Augenheilkunde & Optometrie. Aus unserem Katalog stehen dir über 1 Million Bücher zur Verfügung.
Information
Thema
MedizinBandello F, Souied EH, Querques G (eds): OCT Angiography in Retinal and Macular Diseases.
Dev Ophthalmol. Basel, Karger, 2016, vol 56, pp 45-51 (DOI: 10.1159/000442776)
Dev Ophthalmol. Basel, Karger, 2016, vol 56, pp 45-51 (DOI: 10.1159/000442776)
______________________
Optical Coherence Tomography Angiography of Type 1 Neovascularization in Age-Related Macular Degeneration
Nicholas A. Iafea · Nopasak Phasukkijwatanaa · David Sarrafa, b
aStein Eye Institute, David Geffen School of Medicine at University of California Los Angeles, and bGreater Los Angeles VA Healthcare Center, Los Angeles, Calif., USA
______________________
Abstract
Age-related macular degeneration continues to be the leading cause of severe central vision loss in older adults of European descent. Optical coherence tomography angiography (OCT-A) enables more accurate identification of type 1 neovascularization in age-related macular degeneration than traditional fluorescein and indocyanine green angiographies. In addition, OCT-A facilitates the morphological classification of type 1 lesions, including features characteristic of early, mature, and fibrotic lesions. Vessel complex analysis, including lesion area and capillary density quantification, can also be readily measured and monitored over time. Performing this analysis following anti-vascular endothelial growth factor therapy may lead to a better understanding of the efficacies and responses to such treatments. Although some limitations currently exist, OCT-A is a promising imaging modality that could prove to have profound implications if incorporated into regular clinical practice.
© 2016 S. Karger AG, Basel
Age-related macular degeneration (AMD) continues to be the leading cause of blindness among individuals older than 50 years of age in the developed world [1]. Neovascular AMD is the etiology for severe vision loss in 90% of AMD cases. Three lesion subtypes, best classified on the basis of spectral domain optical coherence tomography (OCT), comprise the neovascular form of this disease [2]. Type 1 neovascularization originates from the choriocapillaris and is localized under the retinal pigment epithelium. Type 2 neovascularization also originates from the choriocapillaris but extends through the retinal pigment epithelium and is localized in the subretinal compartment. Type 3 neovascularization originates from the deep retinal capillary plexus [2-4] and is located in the outer retina. Type 1 neovascularization is the most common neovascular subtype of AMD [5].
Recent advancements in OCT angiography (OCT-A) have provided retinologists with a window to directly identify the morphologies of neovascular subtypes in AMD. OCT-A enables more accurate identification of type 1 lesions compared to traditional fluorescein angiography (FA). While FA can identify the superficial retinal capillary plexus, this imaging modality poorly visualizes the deep retinal capillary plexus and the choroid. Pigment epithelial detachment (PED) may demonstrate pooling or stippled fluorescence with FA, but the identification of the causative neovascular complex is very challenging and only minimally improved with indocyanine green angiography. Conversely, OCT-A utilizes amplitude or phase decorrelation technology with high-frequency and dense volumetric scanning to detect red blood cell movement and to visualize blood vessels at various depth-resolved levels of the retina and choroid [3]. As opposed to FA and indocyanine green angiography, in which the presence of an occult choroidal neovascular membrane is inferred by the presence of pooling within a PED and/or the identification of a hot spot, OCT-A reveals the vessels themselves and enables one to more accurately identify and evaluate the morphology of the neovascular complex.
OCT-A of type 1 neovascularization has lead to a detailed assessment of the microvascular morphologies of these vessel complexes, which are typically hidden under a PED. Numerous studies have identified the different morphologies of these neovascular lesions and have applied varying descriptive terms to label these structures, which are best visualized with OCT-A. These labels include ‘umbrella vessels’ , ‘seafan and medusa vessels’ , ‘tangled network pattern’ , and ‘pruned vascular and blossoming tree’ [3,6,7]. This complicated and indistinct nomenclature has caused confusion in the retina community, and a simpler classification system will certainly evolve that may reflect the chronicity of type 1 neovascularization as identified with OCT-A.
Though the precise precipitating stimulus for angiogenesis in AMD remains to be elucidated, the development of neovascular complexes has been shown to be highly dependent on the presence of vascular endothelial growth factor (VEGF) [8-10]. Hypoperfusion or alteration of the choriocapillaris is often noted in OCT-A in association with type 1 complexes [3,11-13] and is likely one cause of localized increases in VEGF production. The newly established VEGF gradient stimulates the propagation of vascular endothelial cells to form new capillaries [8]. When imaged with OCT-A in this early or acute phase, the neovascularization has the appearance of a tangled web of fine vessels (fig. 1) [8,14]. Muakkassa et al. [14] performed OCT-A on treatment-naïve eyes with type 1 neovascularization, and the lesions were typically small (less than 1 mm2) and comprised of a round tuft of small-caliber capillaries without dilated core feeder vessels.
Chronic type 1 lesions have been noted to demonstrate a distinctly different morphology. In the largest study to date using OCT-A to describe chronic type 1 lesions previously treated with multiple intravitreal anti-VEGF injections, Kuehlewein and associates [3] analyzed 33 eyes with AMD and PED associated with type 1 lesions that were large and mature; these averaged 5.79 mm2 in area. Of note, 75% of the cases showed a highly organized vascular complex with vessels branching from a core trunk (fig. 2) and multiple large, dilated feeder vessels (fig. 3). The existence of well-perfused feeder vessels in chronically treated type 1 lesions has also been identified by Coscas and associates [15]. It has been hypothesized that the feeder vessels and central trunk are more resistant to anti-VEGF therapy because their endothelial cells are protected by overlying pericytes, whereas the finer branching vessels contain unprotected endothelial cells, rendering them more responsive to continued anti-VEGF therapy [16,17]. In his seminal paper, Spaide [8] highlights the distinction between angiogenesis and arteriogenesis and proposes a theory of vascular abnormalization to describe the altered morphology of chronically treated type 1 neovascular complexes. Spaide theorizes that the process of closing smaller pericyte-poor vessels within a neovascular complex in response to anti-VEGF leads to increased vascular resistance within the lesion. The remaining pericyte-rich vessels subsequently experience higher flow and higher intraluminal pressure, thereby creating a stimulus for arteriogenesis and increased vessel size. A cycle of regrowth and pruning of the immature, pericyte-poor vessels at the leading edge of the type 1 complex takes place in response to anti-VEGF therapy, while the mature, dilated pericyte-rich core vessels progressively enlarge. This cycling has been shown to carry a risk of evolution toward subretinal fibrosis [18,19].
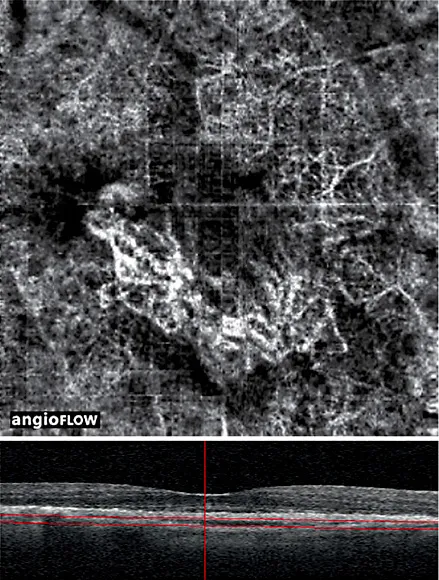
Fig. 1. An 86-year-old patient with treatment-naïve type 1 neovascularization in the right eye. (Top) A 3 mm × 3 mm motion-corrected optical coherence tomography (OCT) angiogram imaged on Avanti RTVue OCTA device showing well-circumscribed choroidal neovascularization with a tangled web of vessels. A quilting artifact due to motion is present. (Bottom) Corresponding spectral domain OCT B-scan with segmentation lines. The authors would like to acknowledge and credit Dr. Nadia Waheed and Dr. Emily Cole for providing these images.
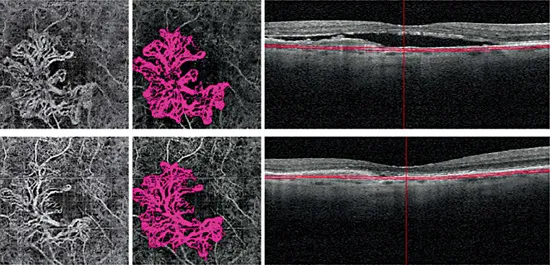
Fig. 2. A 77-year-old male patient with type 1 neovascularization in the right eye, with a visual acuity of 20/40. The patient’s status following 6 aflibercept injections and 7 ranibizumab injections is shown. (Top left) 3 mm x 3 mm OCT angiography (OCT-A) en face projection image of a mature type 1 complex with large feeder vessels and multiple dilated core vessels identified. (Top middle) Corresponding color-coded vessel complex for density analysis. (Top right) OCT B-scan image showing slab segmentation through the pigment epithelial detachment. (Bottom row) Follow-up OCT-A 8 weeks later (interim treatment: 2 aflibercept injections). (Bottom left) 3 mm x 3 mm OCT-A en face projection image of the type 1 complex. (Bottom middle) Corresponding color-coded complex for vessel density analysis. (Bottom right) OCT B-scan image showing slab segmentation. Note that the many large, dilated vessels of this mature type 1 complex are unaffected by additional anti-vascular endothelial growth factor therapy, although the finer vascular plexus may show some attenuation. The lesion area was 3.08 mm2 at baseline and 3.08 mm2 at follow-up; the vessel density was 47% at baseline and 43% at follow-up.
OCT-A has also been employed to study the late fibrotic stage of type 1 neovascularization in AMD. Miere and associates [7] analyzed 49 eyes diagnosed with subretinal fibrosis complicating neovascular AMD, 39 of which were either type 1 or combined type 1 and type 2 lesions. OCT-A demonstrated blood flow related to a persistent neovascular complex within the fibrotic scar in 46 of the 49 eyes [7]. Analysis of these complexes revealed large, dilated vessels with or without vascular loops and interlacing networks, but they typically consisted of only large, mature vessels without an associated fine dense capillary plexus. Most fibrotic lesions also had large flow void areas of the choriocapillaris or dark halos.
Additionally, OCT-A has been utilized to characterize the response of type 1 neovascularization to antiangiogenic therapy. Muakkassa and associates [14] studied six patients with treatment-naïve choroidal neovascularization (CNV), four of which had type 1 lesions. Eyes were scanned before anti-VEGF treatment and at follow-up visits in order to assess the area of each neovascular lesion and its greatest linear dimension (GLD). Follow-up images taken 2-9.5 weeks after initial injection revealed a 29.8% average decrease in CNV area and a 23.6% decrease in its GLD [14]. All patients also experienced improvement or stabilization of...